- Patient Care & Health Information
- Diseases & Conditions
- Cervical cancer
- What is cervical cancer? A Mayo Clinic expert explains
Learn more about cervical cancer from Mayo Clinic gynecologic oncologist Kristina Butler, M.D., M.S.
I'm Dr. Kristina Butler, a gynecologic oncologist at Mayo Clinic. In this video, we'll cover the basics of cervical cancer: What is it? Who gets it? The symptoms, diagnosis, and treatment. Whether you're looking for answers for yourself or someone you love, we're here to give you the best information available. Cervical cancer happens when cells in the cervix, the lower part of the uterus that connects to the vagina, start to become abnormal. Small changes in the cell DNA tells them to multiply out-of-control, and cells accumulate in growths called tumors. Thankfully, advances in medical technology and specifically the use of Pap tests, have significantly helped us identify cervical cancer in patients earlier than ever before. What was once the most common cause of cancer death for American women is now caught sooner and therefore more curable.
While it isn't perfectly clear what sparks the cervical cells to change their DNA, it is certain that human papilloma virus, or HPV, plays a role. HPV is spread by skin to skin contact often during sexual encounters. Over 85% of the general population has been exposed. But most people with HPV never develop cervical cancer. However, reducing your risk of one helps reduce your risk of the other. I recommend getting both the HPV vaccine and regular screening tests. Other risk factors for cervical cancer include multiple sexual encounters. But it only takes one to contract HPV, so it's important to always practice safe sex. A weakened immune system and also smoking are linked to higher risk. One drug called DES was popular in the 1950s as a miscarriage prevention drug. So if your mother took it while pregnant, you may have higher risk as well.
Unfortunately, the early stages of cervical cancer generally show no signs or symptoms. And this is why we emphasize getting Pap smears every three to five years and yearly pelvic exams. Once the cancer has progressed, it can show these symptoms: Unusual vaginal bleeding, for example, after intercourse or between periods or after menopause. Watery, bloody vaginal discharge that may be heavy or have an odor. And pelvic pain or other pain can also occur during intercourse.
Most guidelines suggest starting regular screening for cervical cancer at age 21. And during these screenings, a provider collects cells from the cervix to be tested in the lab. HPV DNA tests examine the cell specifically for HPV that can lead to pre-cancer. A Pap test, or commonly called a Pap smear, tests the cells for abnormalities. The process of these tests are not painful but can be mildly uncomfortable. If your provider suspects cervical cancer, they may start a more thorough examination of the cervix. This may include a colposcopy, which is a special tool that shines light through the vagina into the cervix to magnify the view for your provider. During the colposcopy, your provider might take several deeper samples of cells to examine. This could include a punch biopsy that collects tiny samples of cells, or an endocervical curettage that uses a narrow instrument to take an internal tissue sample. And if after further examination, the sample tissue is worrisome, your doctor may run more tests or collect other tissue samples from deeper layers of the cells. This could use a LEEP or cone biopsy procedure to give the clearest picture possible.
Treating cervical cancer isn't one-size-fits-all. Your doctor will consider the whole picture of your health and your personal preferences before making a recommendation. And this will include one or several treatment methods. For early cervical cancer, we typically treat with surgery to remove the abnormal growths. For more advanced cervical cancer, there's also chemotherapy, a drug that runs the body killing cancer cells in its path. Radiation therapy uses high-powered beams with energy focused on the cancer cells. There's also targeted drug therapy that blocks specific weaknesses present within the cancer cells. And immune therapy, a drug treatment that helps your immune system recognize cancer cells and attack them.
No one can be prepared for a cancer diagnosis. However, there are ways we can help reduce anxiety and feel more in control of the situation. Learning about the condition can make you feel more empowered and confident in the decisions about your care. So ask lots of questions and request additional resources. Find support. Ask for help from your family and friends. If you feel more comfortable expressing yourself in a support group, there are many available both online and in-person. Set goals that you can achieve and feel good about. And most importantly, take care of yourself. This time can be difficult and fatiguing. Eat well, relax and get enough rest. If you'd like to learn even more about cervical cancer, watch our other related videos or visit mayoclinic.org. We wish you well.

Cervical cancer begins in the cells of the cervix.
Cervical cancer is a growth of cells that starts in the cervix. The cervix is the lower part of the uterus that connects to the vagina.
Various strains of the human papillomavirus, also called HPV, play a role in causing most cervical cancers. HPV is a common infection that's passed through sexual contact. When exposed to HPV , the body's immune system typically prevents the virus from doing harm. In a small percentage of people, however, the virus survives for years. This contributes to the process that causes some cervical cells to become cancer cells.
You can reduce your risk of developing cervical cancer by having screening tests and receiving a vaccine that protects against HPV infection.
When cervical cancer happens, it's often first treated with surgery to remove the cancer. Other treatments may include medicines to kill the cancer cells. Options might include chemotherapy and targeted therapy medicines. Radiation therapy with powerful energy beams also may be used. Sometimes treatment combines radiation with low-dose chemotherapy.

Products & Services
- A Book: Mayo Clinic Family Health Book, 5th Edition
- A Book: Taking Care of You

Female reproductive system
The ovaries, fallopian tubes, uterus, cervix and vagina (vaginal canal) make up the female reproductive system.
When it starts, cervical cancer might not cause symptoms. As it grows, cervical cancer might cause signs and symptoms, such as:
- Vaginal bleeding after intercourse, between periods or after menopause.
- Menstrual bleeding that is heavier and lasts longer than usual.
- Watery, bloody vaginal discharge that may be heavy and have a foul odor.
- Pelvic pain or pain during intercourse.
When to see a doctor
Make an appointment with a doctor or other health care professional if you have any symptoms that worry you.
There is a problem with information submitted for this request. Review/update the information highlighted below and resubmit the form.
From Mayo Clinic to your inbox
Sign up for free and stay up to date on research advancements, health tips, current health topics, and expertise on managing health. Click here for an email preview.
Error Email field is required
Error Include a valid email address
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Thank you for subscribing!
You'll soon start receiving the latest Mayo Clinic health information you requested in your inbox.
Sorry something went wrong with your subscription
Please, try again in a couple of minutes

- Where cervical cancer begins
Two types of cells line the surface of the cervix, and both can become cancerous. Glandular cells have a column-shaped appearance. Squamous cells are thin and flat. The boundary between the two types of cells is where most cervical cancers start.
Cervical cancer begins when healthy cells in the cervix develop changes in their DNA . A cell's DNA contains the instructions that tell a cell what to do. The changes tell the cells to multiply quickly. The cells continue living when healthy cells would die as part of their natural life cycle. This causes too many cells. The cells might form a mass called a tumor. The cells can invade and destroy healthy body tissue. In time, the cells can break away and spread to other parts of the body.
Most cervical cancers are caused by HPV . HPV is a common virus that's passed through sexual contact. For most people, the virus never causes problems. It usually goes away on its own. For some, though, the virus can cause changes in the cells that may lead to cancer.
Types of cervical cancer
Cervical cancer is divided into types based on the type of cell in which the cancer begins. The main types of cervical cancer are:
- Squamous cell carcinoma. This type of cervical cancer begins in thin, flat cells, called squamous cells. The squamous cells line the outer part of the cervix. Most cervical cancers are squamous cell carcinomas.
- Adenocarcinoma. This type of cervical cancer begins in the column-shaped gland cells that line the cervical canal.
Sometimes, both types of cells are involved in cervical cancer. Very rarely, cancer occurs in other cells in the cervix.
Risk factors
Risk factors for cervical cancer include:
- Smoking tobacco. Smoking increases the risk of cervical cancer. When HPV infections happen in people who smoke, the infections tend to last longer and are less likely to go away. HPV causes most cervical cancers.
- Increasing number of sexual partners. The greater your number of sexual partners, and the greater your partner's number of sexual partners, the greater your chance of getting HPV .
- Early sexual activity. Having sex at an early age increases your risk of HPV .
- Other sexually transmitted infections. Having other sexually transmitted infections, also called STI s, increases the risk of HPV , which can lead to cervical cancer. Other STI s that increase the risk include herpes, chlamydia, gonorrhea, syphilis and HIV / AIDS .
- A weakened immune system. You may be more likely to develop cervical cancer if your immune system is weakened by another health condition and you have HPV .
- Exposure to miscarriage prevention medicine. If your parent took a medicine called diethylstilbestrol, also known as DES, while pregnant, your risk of cervical cancer might be increased. This medicine was used in the 1950s to prevent miscarriage. It's linked to a type of cervical cancer called clear cell adenocarcinoma.
To reduce your risk of cervical cancer:
- Ask your doctor about the HPV vaccine. Receiving a vaccination to prevent HPV infection may reduce your risk of cervical cancer and other HPV -related cancers. Ask your health care team if an HPV vaccine is right for you.
- Have routine Pap tests. Pap tests can detect precancerous conditions of the cervix. These conditions can be monitored or treated in order to prevent cervical cancer. Most medical organizations suggest beginning routine Pap tests at age 21 and repeating them every few years.
- Practice safe sex. Reduce your risk of cervical cancer by taking measures to prevent sexually transmitted infections. This may include using a condom every time you have sex and limiting the number of sexual partners you have.
- Don't smoke. If you don't smoke, don't start. If you do smoke, talk to a health care professional about ways to help you quit.
More Information
Cervical cancer care at Mayo Clinic
- Cervical cancer FAQs
Living with cervical cancer?
Connect with others like you for support and answers to your questions in the Gynecologic Cancers support group on Mayo Clinic Connect, a patient community.
Gynecologic Cancers Discussions

12 Replies Mon, Apr 15, 2024

4 Replies Thu, Apr 11, 2024
55 Replies Sun, Apr 07, 2024
- Cervical cancer. Cancer.Net. https://www.cancer.net/cancer-types/cervical-cancer/view-all. Accessed March 27, 2023.
- Gershenson DM, et al. Malignant diseases of the cervix. In: Comprehensive Gynecology. 8th ed. Elsevier; 2022. https://www.clinicalkey.com. Accessed March 27, 2023.
- Niederhuber JE, et al., eds. Cancers of the cervix, vulva and vagina. In: Abeloff's Clinical Oncology. 6th ed. Elsevier; 2020. https://www.clinicalkey.com. Accessed March 27, 2023.
- Cervical cancer. National Comprehensive Cancer Network. ps://www.nccn.org/guidelines/guidelines-detail?category=1&id=1426. Accessed March 27, 2023.
- AskMayoExpert. Cervical cancer screening (adult). Mayo Clinic; 2022.
- Palliative care. National Comprehensive Cancer Network. https://www.nccn.org/guidelines/guidelines-detail?category=3&id=1454. Accessed March 27, 2023.
- What is cervical cancer? National Cancer Institute. https://www.cancer.gov/types/cervical. Accessed March 27, 2023.
- Cervical dysplasia: Is it cancer?
- Cone biopsy
Associated Procedures
- Brachytherapy
- Chemotherapy
- Palliative care
- Radiation therapy
News from Mayo Clinic
- Mayo Clinic Minute: Why Black women need to be screened for cervical cancer Jan. 25, 2024, 05:00 p.m. CDT
- Toolkit for reducing cervical cancer risk Jan. 23, 2024, 04:30 p.m. CDT
- Mayo Clinic Minute: Cervical cancer screening Jan. 08, 2024, 03:31 p.m. CDT
- Cervical cancer and HPV -- what's the connection? Jan. 02, 2024, 04:00 p.m. CDT
- Mayo Clinic Health System now offering Saturday appointments for cervical cancer screening June 14, 2023, 05:15 p.m. CDT
- Mayo Clinic Minute: Screening for cervical cancer Jan. 12, 2023, 05:30 p.m. CDT
- Mayo Clinic Q and A: Cervical cancer and HPV screening Jan. 11, 2023, 04:00 p.m. CDT
- 4 ways to reduce risks of cervical cancer Jan. 10, 2023, 03:00 p.m. CDT
Mayo Clinic in Rochester, Minnesota, has been ranked among the best Gynecology hospitals in the nation for 2023-2024 by U.S. News & World Report.
- Symptoms & causes
- Diagnosis & treatment
- Doctors & departments
- Care at Mayo Clinic
Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission.
- Opportunities
Mayo Clinic Press
Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press .
- Mayo Clinic on Incontinence - Mayo Clinic Press Mayo Clinic on Incontinence
- The Essential Diabetes Book - Mayo Clinic Press The Essential Diabetes Book
- Mayo Clinic on Hearing and Balance - Mayo Clinic Press Mayo Clinic on Hearing and Balance
- FREE Mayo Clinic Diet Assessment - Mayo Clinic Press FREE Mayo Clinic Diet Assessment
- Mayo Clinic Health Letter - FREE book - Mayo Clinic Press Mayo Clinic Health Letter - FREE book
Make twice the impact
Your gift can go twice as far to advance cancer research and care!
Skip to Content
- Conquer Cancer
- ASCO Journals
- f Cancer.net on Facebook
- t Cancer.net on Twitter
- q Cancer.net on YouTube
- g Cancer.net on Google
Types of Cancer
- Navigating Cancer Care
- Coping With Cancer
- Research and Advocacy
- Survivorship
Cervical Cancer: Introduction
ON THIS PAGE: You will find some basic information about cervical cancer and the parts of the body it may affect. This is the first page of Cancer.Net’s Guide to Cervical Cancer. Use the menu to see other pages. Think of that menu as a roadmap for this entire guide.
About the cervix
The cervix is the lower, narrow part of the uterus in the female reproductive system. The uterus holds a growing fetus during pregnancy. The cervix connects the lower part of the uterus to the vagina and, with the vagina, forms the birth canal.

About abnormal cells in the cervix that can become cancer
Cervical cancer begins when healthy cells on the surface of the cervix change or become infected with human papillomavirus (HPV) and grow out of control, forming a mass called a tumor. Long-term infection of HPV on the cervix can result in cancer, leading to a mass or tumor on the cervix. A tumor can be cancerous or benign. A cancerous tumor is malignant, meaning it can spread to other parts of the body. A benign tumor means the tumor will not spread.
At first, the changes in a cell are abnormal, not cancerous, and are sometimes called "atypical cells." Researchers believe that some of these abnormal changes are the first step in a series of slow changes that can lead to cancer. Some of the atypical cells go away without treatment, but others can become cancerous. This phase of precancerous disease is called "cervical dysplasia", which is an abnormal growth of cells. Sometimes, the dysplasia tissue needs to be removed to stop cancer from developing. Often, the dysplasia tissue can be removed or destroyed without harming healthy tissue. However, sometimes a hysterectomy is needed to prevent cervical cancer. A hysterectomy is the surgical removal of the uterus and cervix. A loop electrosurgical excision procedure (LEEP) may also be recommended. LEEP uses an electrical current passed through a thin wire hook to remove the tissue.
Treatment of a precancerous area depends on the following factors:
The size of the lesion and the type of changes that have occurred in the cells
The patient's desire to have children in the future
The patient's age and general health
Preferences of the patient and the doctor
If the precancerous cells change into cancer cells and spread deeper into the cervix or to other tissues and organs, the disease is then called cervical cancer or invasive cervical cancer.
About cervical cancer
Cervical cancer can grow from the surface of the cervix seen in the vagina, called the ectocervix, or from the canal going from the vagina to the uterus, called the endocervix. There are 2 main types of cervical cancer named for the type of cell where the cancer started. Other types of cervical cancer are rare.
Squamous cell carcinoma makes up about 80% to 90% of all cervical cancers. These cancers start in the cells on the outer surface covering of the cervix.
Adenocarcinoma makes up 10% to 20% of all cervical cancers. These cancers start in the glandular cells that line the lower birth canal in the internal portion of the cervix.
The squamous and glandular cells meet at the opening of the cervix at the squamocolumnar junction, which is the location where most cervical cancers start.
Looking for More of an Introduction?
If you would like more of an introduction, explore these related items. Please note that these links will take you to other sections on Cancer.Net:
ASCO Answers Fact Sheet: Read a 1-page fact sheet that offers an introduction to cervical cancer. This free fact sheet is available as a PDF, so it is easy to print.
Cancer.Net Blog: Read an American Society of Clinical Oncology (ASCO) expert’s opinion about what newly diagnosed patients should know about gynecologic cancer.
Cancer.Net En Español: Read about cervical cancer in Spanish. Infórmase sobre cancer de cuello uterino en español.
Find a Cancer Doctor. Search for a cancer specialist in your local area using this free database of doctors from the American Society of Clinical Oncology (ASCO).
Cancer Terms. Learn what medical phrases and terms used in cancer care and treatment mean.
The next section in this guide is Statistics . It helps explain the number of people who are diagnosed with cervical cancer and general survival rates. Use the menu to choose a different section to read in this guide.
Cervical Cancer Guide
Cancer.Net Guide Cervical Cancer
- Introduction
- Medical Illustrations
- Risk Factors
- Screening and Prevention
- Symptoms and Signs
- Types of Treatment
- About Clinical Trials
- Latest Research
- Coping with Treatment
- Follow-Up Care
- Questions to Ask the Health Care Team
- Additional Resources
View All Pages
Timely. Trusted. Compassionate.
Comprehensive information for people with cancer, families, and caregivers, from the American Society of Clinical Oncology (ASCO), the voice of the world's oncology professionals.
Find a Cancer Doctor
Cervical cancer
Affiliations.
- 1 Department of Gynaecological Oncology, Bendat Family Comprehensive Cancer Centre, St John of God Subiaco Hospital, Subiaco, Western Australia, WA, Australia; Division of Obstetrics and Gynaecology, Faculty of Health and Medical Sciences, University of Western Australia, Crawley, Western Australia, WA, Australia. Electronic address: [email protected].
- 2 Department of Radiation Oncology, The University of Texas MD Anderson Cancer Center, Houston, Texas, TX, USA.
- 3 Medical Oncology Department, Gynaecological Tumour Unit, Vall d'Hebron University Hospital, Vall d'Hebron, Institute of Oncology (VHIO), Barcelona, Spain.
- 4 Department Obstetrics and Gynaecology, University of Cape Town, Cape Town, South Africa; South African Medical Research Council, Gynaecological Cancer Research Centre, Tygerberg, South Africa.
- PMID: 30638582
- DOI: 10.1016/S0140-6736(18)32470-X
Each year, more than half a million women are diagnosed with cervical cancer and the disease results in over 300 000 deaths worldwide. High-risk subtypes of the human papilloma virus (HPV) are the cause of the disease in most cases. The disease is largely preventable. Approximately 90% of cervical cancers occur in low-income and middle-income countries that lack organised screening and HPV vaccination programmes. In high-income countries, cervical cancer incidence and mortality have more than halved over the past 30 years since the introduction of formal screening programmes. Treatment depends on disease extent at diagnosis and locally available resources, and might involve radical hysterectomy or chemoradiation, or a combination of both. Conservative, fertility-preserving surgical procedures have become standard of care for women with low-risk, early-stage disease. Advances in radiotherapy technology, such as intensity-modulated radiotherapy, have resulted in less treatment-related toxicity for women with locally-advanced disease. For women with metastatic or recurrent disease, the overall prognosis remains poor; nevertheless, the incorporation of the anti-VEGF agent bevacizumab has been able to extend overall survival beyond 12 months. Preliminary results of novel immunotherapeutic approaches, similarly to other solid tumours, have shown promising results so far.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Publication types
- Chemoradiotherapy
- Global Health
- Healthcare Disparities / statistics & numerical data
- Hysterectomy
- Mass Screening / methods
- Mass Screening / statistics & numerical data*
- Neoplasm Staging
- Papillomavirus Infections / epidemiology*
- Papillomavirus Vaccines / immunology
- Risk Factors
- Uterine Cervical Neoplasms* / diagnosis
- Uterine Cervical Neoplasms* / epidemiology
- Uterine Cervical Neoplasms* / prevention & control
- Uterine Cervical Neoplasms* / therapy
- Papillomavirus Vaccines

ESSAY SAUCE
FOR STUDENTS : ALL THE INGREDIENTS OF A GOOD ESSAY
Essay: Cervical cancer
Essay details and download:.
- Subject area(s): Health essays
- Reading time: 21 minutes
- Price: Free download
- Published: 30 December 2017*
- File format: Text
- Words: 5,922 (approx)
- Number of pages: 24 (approx)
Text preview of this essay:
This page of the essay has 5,922 words. Download the full version above.
The causal association between cervical cancer and Human Papilloma Virus (HPV) is one that is well established (3)(4)(5). Thus, prevention strategies are largely targeted at preventing HPV infection or preventing disease progression for those who are infected. There are 2 types of preventive measures available to reduce incidence and mortality from cervical cancer: i.) Vaccination and ii.) Screening. While vaccination is a primary preventive measure (providing protection against the incidence of illness), screening is a secondary preventive measure aiming to diagnose illness early and prevent its progression. Combining screening and vaccination against HPV should potentially provide the best protection against cervical cancer as neither option alone offers 100% protection. At present, screening strategies for cervical cancer have not been altered for females who are HPV vaccinated (6). Screening vaccinated women is arguably still a requirement because of the limitations of current HPV vaccines both in their lack of therapeutic effect (not protecting women with ongoing neoplastic processes) and in their coverage of limited number of HPV types (leaving to evolve some 25–30% of cervical cancer cases related to HPV types other than 16 or 18 strains). Consequently, for health economists, the question regarding the most cost-effective combination of screening strategies along with vaccination arises. The economic impact of screening HPV vaccinated populations is analytical information that health policy makers require for the formulation of effective, evidence-based strategies.
The purpose of this literature review is to collect and collate the best possible evidence available to answer this question. This review aims to systematically analyze health economic studies on HPV vaccination to provide integrated evidence and recommendations based on its cost–effectiveness when combined with differing cervical cancer screening strategies.
Prior Knowledge:
During the search conducted in July 2017, it was noted that a systematic review by Mendes et al (7) on CEA of prevention strategy combinations against HPV infection, was published on March 28th 2017 (after the preliminary literature review search was conducted by the author). Upon examining this paper, it was found that:
i) No quality appraisal of the papers included in the review was carried out.
ii) No papers analyzing the cost effectiveness of screening strategies in populations vaccinated with the non-avalent (9-valent) vaccine (8) were included
iii) The search was finalized in April 2014 resulting in the exclusion of all papers since 2014 till July 2017
iv) The study focused only on studies based in Austria, Belgium, Switzerland, Czech Republic, Germany, Denmark, Spain, Finland, France, Greece, Ireland, Italy, the Netherlands, Norway, Poland, Portugal, Sweden, Slovenia, and the UK, the US, Canada and Australia excluding relevant studies from other parts of the world
Contribution from this literature review:
i) Complete appraisal of all papers using the recommended CHEERS checklist for economic evaluations (9)
ii) A crucial CEA conducted on screening strategies within cohorts vaccinated with the nonavalent or 9-valent vaccine (10)
iii) Studies published after April 2014 were added to this literature review (8) (10)(11)
iv) Relevant studies carried out in Africa (12), Thailand (13), Laos (14), China (15), Taiwan (16) , Israel (17) have been included and reviewed
HPV and Cervical Cancer:
HPV (Human Papilloma Virus) is currently the most common sexually transmitted virus (3). It is passed on primarily through genital contact (such as vaginal and anal sex) and also by skin-to-skin contact (3). Over 100 types of HPV have been identified and more than 40 of these infect the genital area. Although there are several high-risk HPV types, the infection of 2 particular HPV types: 16 and 18 are found to be responsible for 70%–75% of all cervical cancers and 40%–60% of its precursors (18). Among the cancer-related outcomes of HPV infection, cervical cancer is the most important outcome, with over 5,00,000 new cases and 2,75,000 attributable deaths world-wide in 2008 (19). The high-risk (cancer causing) types of HPV include: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 68 (20). Women who are infected with HPV may have their infection clear, progress or persist. Persistence is the most significant determinant of whether or not a HPV-infected woman will develop a clinically significant sequelae (4).
Primary Prevention – Vaccines:
Currently 2 first generation HPV vaccines have enabled prevention against the two most common types of human papillomavirus infection – strains 16, 18 (Bivalent) and also 6 and 11 (Quadrivalent). Clinical trials have provided evidence that the bivalent vaccine was 100% [95% confidential interval (CI) 47–100%, N = 1113] effective against HPV types 16 and 18, and the quadrivalent vaccine 98% [95% CI 86–100%, N = 10,565] (21) (22). These vaccines, have been made available in several countries since their international approval and we are now in the phase of possibly of utilising the second generation of ‘non-avalent’ HPV vaccines (23). These newer vaccines have potential for protection against persistent infection from HPV types 6/11/16/18/31/33/45/52/58 (which together cause ~90% of cervical cancers, globally) (5).
Secondary Prevention – Cervical Cancer Screening Tools:
Persistent HPV infection can cause pre-cancerous cervical lesions and invasive cervical cancer thereafter. With regular cervical cancer screening and appropriate follow-up, most cervical cancer precursors can be identified and treated, interrupting progression to the severe disease stage. Screening programs can reduce cancer risk among those who do not receive the vaccine, those infected by non-vaccine targeted HPV types, and those who demonstrate reduced vaccine efficacy, providing insurance at the population level, given the uncertainties surrounding vaccine performance. The screening tools available include (24):
a.) Cervical Cytology:
Evidence suggests that cervical cancer screening using cytology is one of the most successful public health prevention programs, particularly when implemented in a mass strategy (25). This method involves the collection of exfoliated cells from the cervix followed by microscopic examination of the same after staining, for cellular abnormalities. Based on these abnormalities, further investigation is required to arrive at a diagnosis. There are two cytological screening methods:
i) Conventional PAP smear
ii) Liquid Based Cytology (LBC)
These 2 methods have been extensively compared and it is found that LBC is significantly advantageous in terms of sensitivity and possibility for ‘reflex testing’ of HPV infection without new sample requirements. (26)(27)(28)
b.) Visual Inspection:
Visual inspection of the cervix continues to be implemented as a screening tool for low-resource settings, despite its limited specificity and poor po sitive predictive value (PPV), as it is economical and can provide immediate results. This metho d involves direct visual examination for abnormalities or lesions in the cervix after staining with acetic acid or Lugol’s iodine referred to as Visual Inspection with Acetic Acid (VIA) or Visual Inspection with Lugol’s Iodine (VILI), respectively. (29)
c.) HPV DNA Testing:
Similar to Cytology, HPV DNA testing is done on sample cells collected from the cervix and is used to confirm the presence of infection by the HPV Virus (3)(25). This test has shown higher sensitivity and reproducibility of results than Cytology, for detecting high-grade cervical intraepithelial neoplasia (CIN), (although lower specificity) (30)(31). Unfortunately, the high cost of this option has limited its availability in Low and Middle income countries of the world (32).
Economic Evaluation:
With the costs of healthcare increasing worldwide, there is advancing pressure to ration and efficiently use limited resources. Economic evaluations are utilized to identify, measure, and compare health care intervention costs and benefits, to aid in efficient resource allocation (33).
Economic evaluation, as per the Drummond et. al definition, refers to “the comparative analysis of alternative courses of action in terms of both their costs and consequences” (34). The basic types of economic evaluation include:
1. Cost-benefit analysis (CBA):
CBA measures the benefits and costs of outcomes achieved from an intervention in purely monetary terms. This means that expected years of life gained or expected improvements in health and wellbeing are valued in terms of currency. There is much controversy surrounding CBAs on account of ethical and practical reliability questions on how one may accurately express health outcomes in monetary terms.
2. Cost-effectiveness analysis (CEA):
To overcome the limitations of CBA, CEA was developed as an alternative, more practical approach to healthcare decision-making. It assesses the net cost of a project or service relative to the outcomes generated. CEA is used where the need for a project has already been established, but uncertainty remains over the best method for achieving it (35). The purpose of cost effectiveness analysis is to identify the best method to spend a set budget to achieve a particular goal (36).
3. Cost-utility analysis (CUA):
CUA is often seen as a special form of CEA that introduces measures of benefits that reflect individuals’ preferences over the health consequences of alternative programs that affect them. CUAs use a global measure of health outcome, such as quality-adjusted life-years (QALYs) by undertaking one program instead of another, and the results are often expressed as a cost per QALY gained. (37) This enables the comparison of different types of programs, which makes CUA more practical for decision-makers.
4. Cost-Minimization Analysis (CMA):
Sometimes a cost-minimization analysis is performed if the alternatives under evaluation are considered to achieve the identical health outcomes and carried out in terms of net cost comparisons (38). This specificity of outcome measure reduces its application across health fields, thereby limiting its utilization in evaluation studies.
Source:https://www.ispor.org/PEguidelines/source/Guidelines_Austria.pdf
Economic Modelling:
Full economic analyses of interventions can be carried out by the following approaches:
1. Trial-based studies:
As randomized clinical trials are a necessary condition for the successful licensing of pharmaceuticals, relevant economic data are often obtained alongside the trials for economic evaluations. This method provides internal validity, while the main limitation is that the results may suffer from external generalizability (39).
2. Decision analytic modeling:
This approach brings together a range of evidence sources and allows the expansion of the comparators considered in the analysis and an expansion of the time horizon beyond that of a trial period. Further, decision analytic modeling provides a framework for informing specific decision-making under conditions of uncertainty by allowing more convenient assessment of modeling assumptions, modeling structural uncertainty, and different patient subgroups (heterogeneity) (37). Important model types include:
i) Decision Trees: This is the simplest form of decision analytical modelling in economic evaluation. The pathways in decision trees follow each intervention or process option in a series of logically ordered alternative events, denoted by branches emanating from chance nodes (circular symbols). The alternatives at each chance node must be mutually exclusive and their probabilities sum exactly to one. The end points of each pathway, denoted by terminal nodes (triangular symbols), are assigned values or pay-offs, such as costs, life years, or quality adjusted life years (QALYs). Once the probabilities and pay-offs have been entered, the decision tree is “averaged out” and “folded back” (or rolled back), allowing the expected values of each option to be calculated.
ii) Markov Model: An alternate form of modelling is the Markov model. Unlike decision trees, which represent sequences of events as a large number of complex pathways, Markov models involve simpler and more flexible sequencing of outcomes, including recurring outcomes, through time. Patients are assumed to reside in one of a finite number of health states at any point in time and make transitions between those health states over a series of discrete time intervals or cycles. The probability of staying in a state or moving to another one in each cycle is determined by a set of defined transition probabilities. The definition and number of health states and the duration of the cycles will be governed by the decision problem (40). The final stage is to assign values to each health state, typically costs and health utilities (41)(40). Most commonly, such models simulate the transition of a hypothetical cohort of individuals through the Markov model over time, allowing the analyst to estimate expected costs and outcomes. This simply involves, for each cycle, summing costs and outcomes across health states, weighted by the proportion of the cohort expected to be in each state, and then summing across cycles (42). If the time horizon of the model is over one year, discounting (34) is usually applied to generate the present values of expected costs and outcomes.
iii) Microsimulation models: These models simulate the progression of individuals rather than hypothetical cohorts. They track the progression of potentially heterogeneous individuals with the accumulating history of each individual determining transitions, costs, and health outcome. Unlike Markov models, they can simulate the time to next event rather than requiring equal length cycles and can also simulate multiple events occurring in parallel.
iv) Discrete event simulations: They describe the progress of individuals through healthcare processes or systems, affecting their characteristics and outcomes over unrestricted time periods. These simulations are not restricted to the use of equal time periods or the Markovian assumption and, unlike patient level simulation models, allow individuals to interact with each other.
v) Dynamic models: These models allow internal feedback loops and time delays that affect the behaviour of the entire health system or population being studied. They are particularly valuable in studies of infectious di seases, where analysts may need to account for the evolving effects of factors such as herd im munity on the likelihood of infection over time, and their results can differ substantially from those obtained from static models.
Economic Evaluation Outcomes and Decision rule:
The results of an economic evaluation of an intervention are typically expressed in terms of an ICER – Incremental Cost Effectiveness Ratio. ICERs (measured most often in cost per QALY gained) reflect the incremental cost required to sustain one unit of benefit gained from a particular intervention compared to another. It applies to a decision rule based on a threshold cost effectiveness ratio. This decision rule states that any intervention with a price per unit effectiveness above a fixed threshold, would not be implemented and any program with an ICER below the threshold would be implemented. The threshold that this decision rule is applied to differs between economic settings. The threshold recommended by WHO involves utilizing a value which is a multiple of the GDP of the country under study (43) for cost effectiveness acceptability. An alternative to this is to cite the cost–effectiveness of an intervention that has previously been implemented in the country under study and to utilize the same as a benchmark for acceptable cost–effectiveness. The latter, however, is an approach used mainly in High income countries(43).
The aim of this systematic literature review is to present the comprehensive results of all available international evidence on the cost-effectiveness analysis of different cervical screening strategies for HPV vaccinated populations.
OBJECTIVES:
The main objectives of this review are to:
1) Identify studies conducted to examine cost effectiveness of screening carried out for women post-HPV vaccination.
2) Examine and compare cost effectiveness outcomes of different screening strategies based on frequency, tools implemented and age of primary screening.
3) Conduct a critical appraisal of the literature included for the review.
4) Provide an assessment of the reporting quality of the literature included for the review.
METHODOLOGY:
Ethical Approval:
Ethics approval was first applied for on 31st March 2017 after an initial literature search was conducted to confirm that there were no existing systematic reviews on the topic. Approval was granted by the London School of Hygiene & Tropical Medicine MSc. Research Ethics Committee, on 10th April 2017 (Ethics Ref: 13528 /RR/7584).
PICO Framework:
The P.I.C.O. framework was implemented for the formulation of the appropriate researchable question (44):
Population (P): HPV Vaccinated women
Intervention (I): Screening or vaccination or none
Comparators (C): Comparator screening strategy
Outcome (O): Incremental Cost Effectiveness Ratio
Based on the PICO framework for the research topic, the literature review was then carried out following the PRISMA flowchart in phases of Identification, Screening, Eligibility and Inclusion (45)
Search Strategy:
A comprehensive literature search of peer-reviewed, published journal articles in English was carried out in the standard online databases EMBASE, MEDLINE, PUBMED, NHS EED and Cochrane Library. (NHS EED was not a separate search as it is covered through the Cochrane database (46)). The search strategy was designed using appropriate MeSH and Text words to cover synonyms, combinations and word choices with the main categories which included: 1) Cost effectiveness 2) Screening and 3) HPV Vaccination. This strategy was developed with the help of expert advice from the librarians at the London School of Hygiene & Tropical Medicine. The strategy used for the key words were based on an exploded list of associated MeSH words (identified on PubMed) and free text words, as below:
i. Screening: “Early Diagnosis”, “Early Detection of cancer”, “Screening”,
ii. HPV vaccination: “Papillomavirus Vaccine” “Human Papillomatous Vaccine”, “HPV Vaccine” and “HPV Vaccination”
iii. Cost-effectiveness: “cost effective*” “cost-effective*” “costeffective*” “cost-benefit analysis”, “costbenefit analysis”, “cost benefit analysis”, “cost”, “economic”, “benefit”, “effectiveness”, “Incremental cost-effectiveness analysis”, “Incremental cost-effectiveness ratio”, “ICER”.
Boolean commands of “OR” and “AND” were used appropriately, to join synonyms and string the key words together, respectively (47). The bibliographies of selected publications were scanned and titles cross-referenced to ensure relevant studies were not missed out in the database search.
Study Selection:
All titles of the papers identified were reviewed to filter those which were obviously irrelevant. Following this, the titles and abstracts of remaining papers were reviewed and duplicates were removed. Applying exclusion and inclusion criteria (agreed upon by the author and supervisor) papers with content relevant to the research topic were then isolated. Finally, the citations within these papers were screened thoroughly using the same inclusion criteria to ensure all relevant articles were included for review. The final list of papers identified was then examined in full text, for the data extraction process. The search was completed in July 2017.
Inclusion Criteria:
1. Primary economic evaluations which satisfy the Drummond et al. definition of CEA “the comparative analysis of alternative courses of action in terms of both their costs and consequences”
2. Cost effectiveness analysis (CEA) of different screening strategies combined with HPV vaccination
3. Cost effectiveness analysis with outcome parameters expressed in terms of Incremental Cost Effectiveness Ratio (ICER)
4. Articles in the English language available in full text
Exclusion Criteria:
1. Partial economic analyses (studies that consider either costs or consequences but not both) were not included
2. CEAs of cervical screening between vaccinated and unvaccinated cohorts with no explicit analysis of different screening methods within the vaccinated cohort and only minor variations in the sensitivity analysis were not included.
3. CEAs comparing the same screening strategies combined with different HPV vaccine types, schedules and doses were not included
4. Economic analyses which do not provide outcomes in terms of ICERs were not included
DATA EXTRACTION:
Subsequent to literature identification and screening, the data extraction was conducted by filling in an excel sheet with pre-determined fields which included : Authors’ names, Year of research, Geographical context, Aim, Model implemented, Economic perspective, Vaccine parameters (type, effect duration, dose/ schedule and cost), Screening parameters (tool combinations, frequency and starting age), WTP threshold, Time Horizon, Outcome parameter, Base case results, DSA/ PSA results, Scenario analysis results. Data regarding cost effectiveness of interventions analysing vaccination alone or screening alone was not extracted as it was irrelevant to the research question for this review.
The data extracted was analysed and a narrative description based on their reporting quality, methods and results, grouping them into categories was undertaken.
Quality appraisal:
A quality analysis on reporting of economic evaluations was carried using the recommended CHEERS (Consolidated Health Economic Evaluating Reporting Standards) checklist (9) consisting of 24 items. This checklist was employed because it provides the most relevant criteria for assessing economic evaluations (9) under the subsections of Title and Abstract, Introduction, Methodology, Results and Discussion. The papers were appraised using the checklist version created in Excel and completed in August 2017. Details of the appraisal conducted are attached in the Appendix (Ref. Table No. 2)
Analytical categories:
Owing to high levels of heterogeneity between papers in terms of screening strategy comparisons, modelling methods chosen and geographical context, a descriptive analysis was undertaken. By studying the data extraction tables, papers were then grouped together based on the following broad categories to highlight differences and similarities within these subgroups:
1) ECONOMIC SETTING
2) METHODOLOGICAL APPROACHES
1. Economic perspectives
2. Economic models implemented
3. Outcome measures
4. Cost Effectiveness Thresholds
3) POLICY FINDINGS
1. Screening tool comparisons
2. Screening frequency comparisons
3. Comparisons of varying age of first screening
4. Screening strategies in the context of the nonavalent vaccine
During the search conducted in July 2017, it was noted that a systematic review by Gervais et al. (48) on CEA of prevention strategy combinations against HPV infection, was published on March 28th 2017 (after the preliminary literature review search was conducted by the author). Upon examining this paper, it was found that:
ii) No papers analysing the cost effectiveness of screening strategies in populations vaccinated with the non-avalent (9-valent) vaccine (8) were included
iv) The study included only on studies based in Austria, Belgium, Switzerland, Czech Republic, Germany, Denmark, Spain, Finland, France, Greece, Ireland, Italy, the Netherlands, Norway, Poland, Portugal, Sweden, Slovenia, and the UK, the US, Canada and Australia excluding relevant studies from other parts of the world
ii) 2 crucial CEAs conducted on screening strategies within cohorts vaccinated with the nonavalent or 9-valent vaccine (10)(49)
iii) Studies published after April 2014 were added to this literature review (8)(10)(11)
SEARCH STRATEGY RESULTS:
A total of 1750 studies were identified using the search strategy described above, all of which were examined and filtered to arrive at a final 21 studies which fulfilled all pre-determined inclusion and exclusion criteria illustrated in the PRISMA flow diagram below. The entire search strategy and end results are listed in Table 1 of the Appendix .
PRISMA FLOW DIAGRAM
Quality Appraisal Results:
All of the papers included in this study satisfied most sections in the CHEERS checklist however none of the papers satisfied all of the reporting criteria. Table 2.1 below provides summarized results of the quality appraisal conducted while a detailed extraction is provided in the Appendix Table no. 2. The results demonstrate that the major areas of under-reporting seem to be heterogeneity of populations analysed and currency conversion explanations. It would be important to note that some studies failed to name the type of economic study (i.e. cost effectiveness analysis) in the title, which is essential for proper indexing(50).
TABLE 2.1: Summarized Quality Appraisal Results
(Total n=21)
Articles reporting 100% of CHEERS
checklist items
Missing details:
Title: Economic evaluation description
(8)(51)(52)(15)(10)
Methods: No explicit mention of perspective
Results: Missing reporting of heterogeneity
(53)(51)(54)(55)(56)(57)(52)(58)(59)(16)
(60)(61)(13)(17)(8)(62)(63)(12)(64)
Methods: Missing description of data sources
Methods: Missing description of currency conversion
(10)(53)(51)(54)(55)(56)(57)(52)(58)(59)(16)(15)(17)(8)(62)(60)(61)(14)(49)
Other: Missing source of funding
(63)(53)(52) (59)(16)(17)
Other: Missing conflicts of interest disclosure
ECONOMIC SETTING:
The World bank list of economies, 2016 was used as a reference in labelling the economic setting of the country(65). Contrary to the previous systematic review conducted which only included High income countries, this review included 17 studies based in High Income Countries (HIC’s) while the remaining 4 were based in Low (14)(12) and Middle (15)(13) Income Countries (LMIC’s).
METHODOLOGICAL APPROACHES:
1) Economic perspectives:
From the review conducted, it was found that only 7 studies (17) (10) (53) (23) (11) (64) (61) adopted the Health Service perspective by including only direct medical costs of vaccination, screening and cervical cancer treatment borne by the paying party. The remaining 14 studies adopted the Societal perspective including both direct and indirect medical costs associated with vaccination, screening and cervical cancer treatment.
2) Decision analytical models implemented:
i.) Markov Model: 8 out of the 21 studies (53)(51)(57)(52)(59)(16)(13)(17) included implemented the Markov Model
ii.) Microsimulation model: 5 studies implemented the Microsimulation model (54)(55)(56)(8)(60) all of which were in high income settings and suggested HPV DNA testing as a cost-effective tool for cervical screening among HPV vaccinated cohorts with varying age of initiation and intervals for screening.
iii.) Dynamic model: Only 3 studies implemented the Dynamic model (10)(14)(49)
iv.) More than one model: A total of 5 studies implemented more than one analytical model using hybrid combinations of a transmission cum disease history model (61)(58), dynamic cum cohort simulation models (15), dynamic model cum deterministic multi-cohort model (11) and natural history cum cohort simulation models (12).
3) Outcome measures:
i. Cost/QALY: 9 of the studies expressed the ICER in terms of Cost Per Quality Adjusted Life Year (QALY) gained (53)(51)(58)(57)(56)(8)(60)(61)(49)
ii. Cost/YLS: 9 of the studies expressed the ICER in Cost Per Year of Life Saved (YLS) (54)(55)(52)(66)(15)(13)(11)(10)(12)
iii. Cost/DALY averted: 2 studies expressed the ICER as Cost / DALY averted (17)(14)
iv. Cost/ QALE: 1 study alone expressed the ICER as Cost / Quality Adjusted Life Expectancy (59)
The choice to represent the ICER in Cost per QALY gained was carried out in all High Income Country settings while the 2 studies with ICERs in Cost per DALY averted were in one Low income setting (63) and one high income setting (17). 9 studies which used Cost per YLS to represent the ICER, were from HIC (54)(55)(52)(66)(15)(10)(11) and 2 were from LMIC (12)(13) settings.
4) Willingness To Pay or Cost-Effectiveness thresholds:
The threshold values adopted for Cost Effectiveness included the:
i) WHO recommendation(34) of 1 to 3 times GDP (54)(15)(13)(17)(60) (61)(14)(12)
ii) Country specific accepted thresholds (59)(58)(52)(57)(56)(55)(51)(53) (16)(8)(10)
Only one study did not specify the threshold adopted in their analysis (11).
POLICY FINDINGS:
1) Screening Tool comparisons:
Different screening tools and tool combination comparisons were made in 10 of the studies reviewed (54)(55)(56)(67)(66)(8)(11)(60)(63)(12). For example, the study by Kim et al (54) examined the cost effectiveness of Cytology alone, Cytology with HPV DNA triage and co-testing with Cytology & HPV DNA while the study by Lew et al (11) examines Conventional cytology, Manually-read liquid-based cytology, Image-read liquid-based cytology, HPV Testing with liquid-based cytology triaging, HPV testing with partial genotyping for HPV 16/18 and liquid-based cytology triaging, Co-testing with both HPV Testing and Liquid based cytology.
2) Screening frequency comparisons:
Cost effectiveness analysis by comparing different intervals between screenings was carried out in all of the studies included for review. The intervals were varied in terms of number of years of gap between one screening strategy in all of the studies except for 3: in which different intervals were applied to different screening tools (17), different intervals were applied to different age groups (11) and different intervals applied to different vaccines types (60) were examined.
3) Comparisons between age of screening implementation:
Different ages of screening initiation and cessation were evaluated in all studies included, except for 3 (66)(13)(58). 9 studies included assessed cost effectiveness cohorts by varying age of initiation of screening alone after vaccination (61)(63)(53)(51)(54)(55)(56)(57)(52)(8). One study by Coupé et al (60), in contrast, examined 3 scenarios with age variations for vaccines of different valences and doses concluding that 4 rounds of HPV DNA screening between 30 and 60 years of age for bivalent vaccine and one lifetime screening for broad spectrum vaccinations proved cost effective in the Netherlands.
4) Screening strategies in the context of HPV 9 / Nonavalent vaccine:
Two crucial studies included in this review (which were not part of the review by Gervais et al. (48)) examine the cost effectiveness of screening women vaccinated with the new nonavalent HPV vaccine in HIC settings.
i.) The study by Simms et al, August 2016 (10) implemented a well-validated dynamic model of HPV transmission and cervical screening incorporating the influence of vaccination, herd immunity and screening. The authors concluded that if the intensity of screening programs is significantly less per woman’s lifetime (post vaccination), screening will remain cost-effective once the nonavalent vaccine is implemented.
ii.) The study by Simms et al, December 2016 (49), examined the cost effectiveness of screening Nonavalent vaccinated cohorts compared to HPV 4 vaccinated cohorts. The authors concluded that screening of the former group proves cost effective, compared to the latter, provided the additional cost per vaccine dose remains between 23 and 36 AUS$.
5) Analysis of the effect of Herd Immunity:
Notably, most of the studies did not account for heterogeneity of the population examined except for 2 which examined the effects of herd immunity within vaccinated populations. Areas worthy of exploring heterogeneity could include population subgroups of varying socio-economic backgrounds, risk exposure viz.: multiple sexual partners or previous history of sexually transmitted infections.
The entire data extraction table built and developed for the purpose of this review is provided in the Appendix in Table 3, for further reference.
DISCUSSION:
In total, 21 studies (available in full text format) published until July 2017 in peer reviewed journals were included in the review. All of the papers were described in the abstracts as cost-effectiveness analyses. The data gathered from the papers are discussed below following the thematic sequence of the results demonstrated above.
QUALITY APPRAISAL:
The CHEERS checklist is recommended for the appraisal of economic evaluations with the aim of providing set guidelines to authors, editors and reviewers to improve reporting standards (50). The studies included in this review were found to be of high quality fulfilling most of the reporting criteria.
Title Quality:
The title of the paper is required to identify the study as an economic evaluation and preferably also mention the type of economic evaluation conducted. This is primarily for the purpose of ensuring the studies are indexed appropriately (50) and there are less chances of the studies being missed by reviewers. 5 studies included in this study failed to provide an accurate title requiring the author to examine the abstract to confirm if indeed it was an economic evaluation.
Abstract Reporting Quality:
CHEERS recommends the use of ‘structured’ abstracts as studies have proven that these provide higher reporting quality than descriptive abstracts, which allows readers to locate relevant information easier (68)(69). While all studies provided structured abstracts, only one study out of 21 provided a structured summary by mentioning all of the specified headings: objectives, perspective, setting, methods (including study design and inputs), results (including base-case and uncertainty analyses) and conclusions.
Quality of Introduction:
This section is expected to provide an explicit statement and explanation of the broad context of the study and its relevance in health policy. This checklist item was scrutinized in conjunction with checklist items 4 till 7 i.e. target population and subgroups, setting and location, study perspective and comparators, as recommended (50). All of the studies included in this review were found to satisfy the reporting standards for the introduction.
Qual ity of Reporting Methods:
i) Target population and subgroups: Definition of population groups under evaluation is of particular importance in economic studies as cost-effectiveness results vary by cohort characteristics (70). All the studies in this review were found to provide a detailed explanation of population characteristics with respect to demographic profiles, vaccine coverage or uptake rates, follow-up visit adherence, etc. and explained reasons for assumptions regarding vaccine efficacy, screening coverage etc.
ii) Setting and Location: All studies clearly described the system within which the vaccine and screening interventions were being provided. This ensures that the evaluation undertaken addressed the question relevant to the population setting.
iii) Study Perspective: All evaluations made clear mention of the economic perspective implemented and provided reasons for the choice and costs included, except for one study by Sopina et al, for which the author derived the perspective by examining the costs included.
iv) Time Horizon: Since only preventive interventions were examined in these analyses, they are particularly sensitive to the time horizon (71) owing to influencing factors such as waning of immunity from vaccination, protection from herd immunity with increased coverage, discounting etc. All the studies provided a description of time horizon choice. It was specially noted that all studies utilizing the dynamic model provided explanations for time horizon chosen, as this model is known to be sensitive to this parameter.
v) Measurement of preference based outcomes and data sources: All studies provided specific mention of the preference-based outcome measurements and other data sources except for one by Goldie et al (57), which did not include clear mention of preference-elicitation techniques (e.g. EuroQoL5D), data sources or methods for extrapolating data from published studies.
vi) Reporting of heterogeneity and currency conversion: It is recommended that authors must report differences in costs, outcomes, or cost-effectiveness that can be explained by variation between subgroup characteristics of patients such as age, socio-economic background, co-morbidities etc. The reasons for heterogeneity were poorly touched upon in a majority of studies here. This could be due to poor quality and/or lack of data available, incompatibility with model type to incorporate heterogeneity influences, etc. The cause for poor reporting of currency conversion, on the other hand, could be due to lack of consistent or set guidelines for reporting these elements.
Missing Generalizability Description:
None of the studies included in this review explicitly accounted for generalizability of their results although the findings, limitations and current knowledge explanations were discussed in detail. Economic evaluations must pay particular attention to this criterion on account of the fact that if they are set with a particular jurisdiction in mind, it would be inappropriate to use the findings in a different setting (E.g., LMIC and HIC settings). Authors should ideally, explicitly discuss how findings can and cannot be applied to local or global settings to avoid errors in evidence-based policy formulation.
Missing source of funding and conflict of interest disclosure:
Some of the studies failed to disclose all sources of funding (funds received both directly and indirectly) which limit credibility. This is because studies funded by pharmaceutical companies, for example, may only be interested in publishing findings that may be in favour of interventions requiring products manufactured by them as against non-commercial funders. It is advised that the ICJME recommendations (72) are followed for declaration of conflicts of interest by the authors even when there are no conflicts to ensure transparency and credibility.
This review included all papers relevant to the research question irrespective of the geographic setting of the analysis, in contrast to the review by Gervais et. al (48). Comparative analysis of economic evaluations across diverse economic resource settings are known to be challenging but in accordance with the pattern observed by Griffiths et al (73) it was found that studies in Low and Middle income countries relied upon micro-costing method for cost data while those in High income countries utilized Gross costing based on national administrative databases.
Choice of Economic Perspective:
Majority of the studies chose the Societal perspective. None of the LMIC based studies utilized the Health service perspective except for one (63) study based in Lao. This is in agreement with the guidelines used by researchers in LMIC’s (73)(74) which state the preferred perspective would be Societal except in Egypt). Adopting a societal perspective, including all direct and indirect costs and benefits, facilitates policies aimed at maximising the welfare gains to society, or minimising the losses (75). However, in practice, it is not always feasible to include all possible costs and benefits in an economic evaluation which is why the health service perspective is popular among researchers. In the context of this review, the use of different perspectives poses a limitation towards comparability of the studies included.
Choice of Decision Analytical model:
Decision modelling for Cervical Cancer is particularly challenging as it involves incorporating elements of both an infectious disease (HPV infection) as well as a chronic illness (Cervical Carcinoma). As there are no clearly defined guidelines on choice of decision model and limited guidance on good modelling (76) each model type examined in this review is discussed in the context of the illness under study. The majority of studies reviewed implemented the Markov Model, all of which make clear their source of cost, utility and transition probability data. This model is simple to develop and is ideal for chronic disease conditions. However, the studies using this model faced the limitation that interaction between individuals or groups (e.g. herd immunity) cannot be accounted for, different characteristics of individuals / groups cannot be incorporated and resource constraints cannot be considered (77). Some studies implemented the Dynamic model, which requires a great volume of parameters and advanced statistical programming knowledge. It is best suited for strategies aimed at controlling infectious diseases. This allows for studying interactions between individuals / groups and estimation of direct and indirect effects of interventions (e.g. herd immunity) (77)(78)(49). The studies which implemented the Microsimulation Model benefited from being able to incorporate individual characteristics changing over time, resource constraints and allowing for random events (77).
...(download the rest of the essay above)
About this essay:
If you use part of this page in your own work, you need to provide a citation, as follows:
Essay Sauce, Cervical cancer . Available from:<https://www.essaysauce.com/health-essays/cervical-cancer/> [Accessed 12-04-24].
These Health essays have been submitted to us by students in order to help you with your studies.
* This essay may have been previously published on Essay.uk.com at an earlier date.
Essay Categories:
- Accounting essays
- Architecture essays
- Business essays
- Computer science essays
- Criminology essays
- Economics essays
- Education essays
- Engineering essays
- English language essays
- Environmental studies essays
- Essay examples
- Finance essays
- Geography essays
- Health essays
- History essays
- Hospitality and tourism essays
- Human rights essays
- Information technology essays
- International relations
- Leadership essays
- Linguistics essays
- Literature essays
- Management essays
- Marketing essays
- Mathematics essays
- Media essays
- Medicine essays
- Military essays
- Miscellaneous essays
- Music Essays
- Nursing essays
- Philosophy essays
- Photography and arts essays
- Politics essays
- Project management essays
- Psychology essays
- Religious studies and theology essays
- Sample essays
- Science essays
- Social work essays
- Sociology essays
- Sports essays
- Types of essay
- Zoology essays
Advertisement
Improving cervical cancer continuum of care towards elimination in Ethiopia: a scoping review
- Published: 04 November 2023
- Volume 35 , pages 549–559, ( 2024 )
Cite this article
- Aklilu Endalamaw 1 , 2 ,
- Habtamu Alganeh 2 ,
- Muluken Azage 2 ,
- Asmamaw Atnafu 3 ,
- Daniel Erku 4 , 5 ,
- Eskinder Wolka 6 ,
- Adane Nigusie 3 ,
- Anteneh Zewdie 6 ,
- Destaw Fetene Teshome 3 &
- Yibeltal Assefa 1
408 Accesses
Explore all metrics
Cervical cancer is the second-leading cause of death among all cancers in Ethiopia. Ethiopia plans to eliminate cervical cancer as a public health problem by 2030, following the World Health Organization's call for action. A scoping review was conducted on the status of the cervical cancer continuum towards elimination in Ethiopia.
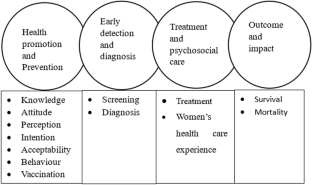
We searched articles in PubMed, Scopus, and Google Scholar. All studies conducted on cervical cancer in Ethiopia, from first date of publication to March 15, 2023, type of article, or language of publication, were included. However, conference abstracts, commentaries, and letters to the editors were excluded. We used EndNote X9 software to merge articles from different databases and automatically remove duplicates. Screening of titles, abstracts, and full texts was performed independently by two co-authors. The cancer care continuum was employed as a framework to guide data synthesis and present the findings.
Of the 569 retrieved articles, 159 were included in the review. They found that most of the articles focused on knowledge, attitude, and practice. However, there were few studies on health-seeking behavior, perception and acceptability of cervical cancer services, as well as the availability and readiness of a screening program. The review identified inadequate knowledge, attitude, and perception about cervical cancer, and highlighted that screening for cervical cancer is not widely utilized in Ethiopia. Knowledge, attitude, education status, and income were repeatedly reported as precursors influencing cervical cancer screening. Most studies concluded that there is a high prevalence of precancerous lesions and cervical cancer, as well as high mortality rates or short survival times. The review also identified significant heterogeneity in findings across time and geographic settings within each component of the cancer care continuum.
Conclusions
Overall, there is inadequate knowledge, perception, health-seeking behavior, screening, and treatment services, indicating that the country is falling behind its targets in eliminating cervical cancer, despite the availability of effective interventions and tools. We argue that implementation research is necessary to identify implementation issues, challenges, and strategies to scale up both primary and secondary prevention services. By doing so, Ethiopia can address cervical cancer as a public health problem and work towards its elimination.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
Similar content being viewed by others

Disparities in cervical cancer screening programs in Cameroon: a scoping review of facilitators and barriers to implementation and uptake of screening
Namanou Ines Emma Woks, Musi Merveille Anwi, … Angel Phuti

Barriers to uptake of cervical cancer screening services in low-and-middle-income countries: a systematic review
Z. Petersen, A. Jaca, … S. Moyo

Persistent cervical cancer disparities among American Indian/Alaska Native women: a systematic scoping review exploring the state of the science in this population
Katherine C. Fitch, Christine G. T. Nguyen, … Amanda S. Bruegl
Data availability
All the generated data are available within this manuscript.
Abbreviations
Human immunodeficiency virus
Human papilloma virus
Southern Nation Nationalities People Region
United States Dollar
Visual inspection with acetic acid
World Health Organization
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A et al (2021) Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71(3):209–249
Article PubMed Google Scholar
Ginsburg O, Bray F, Coleman MP, Vanderpuye V, Eniu A, Kotha SR et al (2017) The global burden of women’s cancers: a grand challenge in global health. Lancet 389(10071):847–860
Arbyn M, Weiderpass E, Bruni L, de Sanjosé S, Saraiya M, Ferlay J et al (2020) Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health 8(2):e191–e203
Bruni L, Albero G, Serrano B, Mena M, Collado JJ, Gómez D, Muñoz J, Bosch FX, de Sanjosé S (2023) ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in Ethiopia. Summary Report 10 March 2023
Zhang X, Zeng Q, Cai W, Ruan W (2021) Trends of cervical cancer at global, regional, and national level: data from the Global Burden of Disease study 2019. BMC Public Health 21(1):1–10
Google Scholar
Kocarnik JM, Compton K, Dean FE, Fu W, Gaw BL, Harvey JD et al (2022) Cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life years for 29 cancer groups from 2010 to 2019: a systematic analysis for the global burden of disease study 2019. JAMA Oncol 8(3):420–444
Abbas KM, van Zandvoort K, Brisson M, Jit M (2020) Effects of updated demography, disability weights, and cervical cancer burden on estimates of human papillomavirus vaccination impact at the global, regional, and national levels: a PRIME modelling study. Lancet Glob Health 8(4):e536–e544
Article PubMed PubMed Central Google Scholar
World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem 2020. https://www.who.int/publications/i/item/9789240014107
The Economist Intelligence Unit. Global action on financing cervical cancer elimination Funding secondary prevention services in low resource settings 2020. https://www.eiu.com/default.aspx
Union for International Cancer Control Cervical Cancer: a unique opportunity to work towards equity. https://www.uicc.org/what-we-do/driving-global-impact/targeted-commitments/cervical-cancer-elimination-strategy?gclid=CjwKCAjwoIqhBhAGEiwArXT7KxW6k5wQhHRpuApNn9os7N9GIyzf8aGvvZcr6IVdr-ccOihGV0PTGxoC_AUQAvD_BwE#49619
Lakneh EA, Mersha EA, Asresie MB, Belay HG (2022) Knowledge, attitude, and uptake of human papilloma virus vaccine and associated factors among female preparatory school students in Bahir Dar City, Amhara Region, Ethiopia. PLoS One 17(11):e0276465
Article CAS PubMed PubMed Central Google Scholar
Larebo YM, Elilo LT, Abame DE, Akiso DE, Bawore SG, Anshebo AA et al (2022) Awareness, acceptance, and associated factors of human papillomavirus vaccine among parents of daughters in Hadiya zone, southern Ethiopia: a cross-sectional study. Vaccines 10(12):1988
(DCCPS) DoCCaPS (2020) Cancer Control Continuum: National Cancer Institute. https://cancercontrol.cancer.gov/about-dccps/about-cc/cancer-control-continuum
Bekele HT, Nuri A, Abera L (2022) Knowledge, attitude, and practice toward cervical cancer screening and associated factors among college and university female students in Dire Dawa City, Eastern Ethiopia. Cancer Inform 21:11769351221084808
Mruts KB, Gebremariam TB (2018) Knowledge and perception towards cervical cancer among female Debre Berhan University students. Asian Pac J Cancer Prev 19(7):1771–1777
PubMed PubMed Central Google Scholar
Abebaw E, Tesfa M, Gezimu W, Bekele F, Duguma A (2022) Female healthcare providers’ knowledge, attitude, and practice towards cervical cancer screening and associated factors in public hospitals of Northwest Ethiopia. SAGE Open Med 10:20503121221095931
Ararsa T, Tadele N, Ayalew Y, Gela D (2021) Knowledge towards cervical cancer screening and associated factors among urban health extension workers at Addis Ababa, Ethiopia: facility based cross-sectional survey. BMC Cancer 21(1):224
Erku DA, Netere AK, Mersha AG, Abebe SA, Mekuria AB, Belachew SA (2017) Comprehensive knowledge and uptake of cervical cancer screening is low among women living with HIV/AIDS in Northwest Ethiopia. Gynecol Oncol Res Pract 4:20
Dulla D, Daka D, Wakgari N (2017) Knowledge about cervical cancer screening and its practice among female health care workers in Southern Ethiopia: a cross-sectional study. Int J Women’s Health 9:365–372
Article Google Scholar
Mengesha A, Messele A, Beletew B (2020) Knowledge and attitude towards cervical cancer among reproductive age group women in Gondar town, North West Ethiopia. BMC Public Health 20(1):209
Tsegay A, Araya T, Amare K, Gtsadik F (2021) Knowledge, attitude, and practice on cervical cancer screening and associated factors among women aged 15–49 years in Adigrat Town, Northern Ethiopia, 2019: a Community-Based Cross-Sectional Study. Int J Women’s Health 2021:1283–1298
Tilahun T, Tulu T, Dechasa W (2019) Knowledge, attitude and practice of cervical cancer screening and associated factors amongst female students at Wollega University, western Ethiopia. BMC Res Notes 12(1):518
Tadesse A, Tafa Segni M, Demissie HF (2022) Knowledge, Attitude, and Practice (KAP) toward Cervical Cancer Screening among Adama Science and Technology University Female Students, Ethiopia. Int J Breast Cancer 2022
Tafere Y, Jemere T, Desalegn T, Melak A (2021) Women’s knowledge and attitude towards cervical cancer preventive measures and associated factors in South Gondar Zone, Amhara Region, North Central Ethiopia: a cross-sectional study. Arch Public Health 79(1):136
Gebisa T, Bala ET, Deriba BS (2022) Knowledge, attitude, and practice toward cervical cancer screening among women attending health facilities in central Ethiopia. Cancer Control 29:10732748221076680
Aweke YH, Ayanto SY, Ersado TL (2017) Knowledge, attitude and practice for cervical cancer prevention and control among women of childbearing age in Hossana Town, Hadiya zone, Southern Ethiopia: community-based cross-sectional study. PLoS One 12(7):e0181415
Demissie BW, Azeze GA, Asseffa NA, Lake EA, Besha BB, Gelaw KA et al (2022) Communities’ perceptions towards cervical cancer and its screening in Wolaita zone, southern Ethiopia: a qualitative study. PLoS One 17(1):e0262142
Birhanu Z, Abdissa A, Belachew T, Deribew A, Segni H, Tsu V et al (2012) Health seeking behavior for cervical cancer in Ethiopia: a qualitative study. Int J Equity Health 11(1):1–8
Mesafint Z, Berhane Y, Desalegn D (2018) Health seeking behavior of patients diagnosed with cervical cancer in Addis Ababa, Ethiopia. Ethiop J Health Sci 28(2):111–116
Habtu Y, Yohannes S, Laelago T (2018) Health seeking behavior and its determinants for cervical cancer among women of childbearing age in Hossana Town, Hadiya zone, Southern Ethiopia: community based cross sectional study. BMC Cancer 18(1):298
Wollancho W, Amdissa D, Bamboro S, Wasihun Y, Tareke KG, Gizaw AT (2020) Determining behavioral intention and its predictors towards cervical cancer screening among women in Gomma district, Jimma, Ethiopia: application of the theory of planned behavior. PLoS One 15(11):e0238472
Alemnew W, Debalkie G, Azale T (2020) Intention to screen for cervical cancer among child bearing age women in Bahir Dar City, North-West Ethiopia: using theory of planned behavior. Int J Women’s Health 2020:1215–1222
Eshetu HB, Shitu K, Handebo S (2022) Predictors of intention to receive cervical cancer screening among commercial sex workers in Gondar city, northwest Ethiopia: application of the theory of planned behavior. BMC Womens Health 22(1):462
Mihretie GN, Liyeh TM, Ayele AD, Belay HG, Yimer TS, Miskr AD (2022) Knowledge and willingness of parents towards child girl HPV vaccination in Debre Tabor Town, Ethiopia: a community-based cross-sectional study. Reprod Health 19(1):136
Dereje N, Ashenafi A, Abera A, Melaku E, Yirgashewa K, Yitna M et al (2021) Knowledge and acceptance of HPV vaccination and its associated factors among parents of daughters in Addis Ababa, Ethiopia: a community-based cross-sectional study. Infect Agent Cancer 16(1):58
Beyen MW, Bulto GA, Chaka EE, Debelo BT, Roga EY, Wakgari N et al (2022) Human papillomavirus vaccination uptake and its associated factors among adolescent school girls in Ambo town, Oromia region, Ethiopia, 2020. PLoS One 17(7):e0271237
Kassa HN, Bilchut AH, Mekuria AD, Lewetie EM (2021) Practice and associated factors of human papillomavirus vaccination among primary school students in Minjar-Shenkora District, North Shoa Zone, Amhara Regional State, Ethiopia, 2020. Cancer Manag Res 13:6999–7008
Aragaw GM, Anteneh TA, Abiy SA, Bewota MA, Aynalem GL (2023) Parents’ willingness to vaccinate their daughters with human papillomavirus vaccine and associated factors in Debretabor town, Northwest Ethiopia: a community-based cross-sectional study. Hum Vaccines Immunother 2023:2176082
Ukumo EY, Weldehawariat FG, Dessalegn SA, Minamo DM, Weldehawaryat HN (2022) Acceptance of human papillomavirus vaccination and associated factors among girls in Arba Minch Town, Southern Ethiopia, 2020. Infect Dis Obstet Gynecol 2022:7303801
Alene T, Atnafu A, Mekonnen ZA, Minyihun A (2020) Acceptance of human papillomavirus vaccination and associated factors among parents of daughters in Gondar Town, Northwest Ethiopia. Cancer Manag Res 12:8519–8526
Biyazin T, Yetwale A, Fenta B (2022) Willingness to accept human papillomavirus vaccination in Jimma town, Ethiopia. Hum Vaccin Immunother 18(6):2125701
Desta M, Getaneh T, Yeserah B, Worku Y, Eshete T, Birhanu MY et al (2021) Cervical cancer screening utilization and predictors among eligible women in Ethiopia: a systematic review and meta-analysis. PLoS One 16(11):e0259339
Dessalegn MB (2020) Cervical cancer screening uptake and associated factors among HIV-positive women in Ethiopia: a systematic review and meta-analysis. Adv Prev Med 2020:7071925
Argaw M, Embiale A, Amare B (2022) Knowledge, and practice of cervical cancer prevention and associated factors among commercial sex workers in Shashemene Town, West Arsi, Oromia Region, Ethiopia. BMC Womens Health 22(1):233
Wasiyhun TS, Beyene MG, Deghebo AD, Getachew T, Zeleke GT, Tesema TT et al (2021) Availability and readiness of cervical cancer screening service at health facilities in Ethiopia. Ethiop J Public Health Nutr 4(2):141
Jede F, Brandt T, Gedefaw M, Wubneh SB, Abebe T, Teka B et al (2020) Home-based HPV self-sampling assisted by a cloud-based electronic data system: Lessons learnt from a pilot community cervical cancer screening campaign in rural Ethiopia. Papillomavirus Res 9:100198
de Fouw M, Kaba M, Hailu M, Bereket FZ, Beltman JJ (2019) Local community networks in the fight against cervical cancer: the role of coffee ceremonies in the uptake of screening in Ethiopia. Trop Doct 49(4):298–300
Abu SH, Woldehanna BT, Nida ET, Tilahun AW, Gebremariam MY, Sisay MM (2020) The role of health education on cervical cancer screening uptake at selected health centers in Addis Ababa. PLoS One 15(10):e0239580
Shiferaw N, Salvador-Davila G, Kassahun K, Brooks MI, Weldegebreal T, Tilahun Y et al (2016) The single-visit approach as a cervical cancer prevention strategy among women with HIV in Ethiopia: successes and lessons learned. Glob Health Sci Pract 4(1):87–98
Assefa T, Arefaynie M, Mebratu W, Mohammed A, Addisu E, Kebede N (2022) Determinants of cervical cancer screening utilization among women attending health facilities of Dessie town, Northeast Ethiopia. BMC Cancer 22(1):1330
Ayenew AA, Zewdu BF, Nigussie AA (2020) Uptake of cervical cancer screening service and associated factors among age-eligible women in Ethiopia: systematic review and meta-analysis. Infect Agent Cancer 15(1):67
Midaksa M, Destaw A, Addissie A, Kantelhardt EJ, Gizaw M (2022) Women’s sexual autonomy as a determinant of cervical cancer screening uptake in Addis Ababa, Ethiopia: a case–control study. BMC Womens Health 22(1):236
Lott BE, Halkiyo A, Kassa DW, Kebede T, Dedefo A, Ehiri J et al (2021) Health workers’ perspectives on barriers and facilitators to implementing a new national cervical cancer screening program in Ethiopia. BMC Womens Health 21(1):1–14
Megersa BS, Bussmann H, Bärnighausen T, Muche AA, Alemu K, Deckert A (2020) Community cervical cancer screening: barriers to successful home-based HPV self-sampling in Dabat district, North Gondar, Ethiopia. A qualitative study. PLoS One 15(12):e0243036
Temesgen MM, Alemu T, Shiferaw B, Legesse S, Zeru T, Haile M et al (2021) Prevalence of oncogenic human papillomavirus (HPV 16/18) infection, cervical lesions and its associated factors among women aged 21–49 years in Amhara region, Northern Ethiopia. PLoS One 16(3):e0248949
Fentie AM, Tadesse TB, Gebretekle GB (2020) Factors affecting cervical cancer screening uptake, visual inspection with acetic acid positivity and its predictors among women attending cervical cancer screening service in Addis Ababa, Ethiopia. BMC Womens Health 20(1):147
Mekuria M, Edosa K, Endashaw M, Bala ET, Chaka EE, Deriba BS et al (2021) Prevalence of cervical cancer and associated factors among women attended cervical cancer screening center at Gahandi Memorial Hospital, Ethiopia. Cancer Inform 20:11769351211068432
Getinet M, Taye M, Ayinalem A, Gitie M (2021) Precancerous lesions of the cervix and associated factors among women of East Gojjam, Northwest Ethiopia, 2020. Cancer Manag Res 13:9401–9410
Belayneh T, Mitiku H, Weldegebreal F (2019) Precancerous cervical lesion and associated factors among HIV-infected women on ART in Amhara Regional State, Ethiopia: a hospital-based cross-sectional study. Int J Health Sci (Qassim) 13(3):4–9
PubMed Google Scholar
Pelzer A, Duncan ME, Tibaux G, Mehari L (1992) A study of cervical cancer in Ethiopian women. Cytopathology 3(3):139–148
Article CAS PubMed Google Scholar
Zelalem W, Weldegebreal F, Ayele BH, Deressa A, Debella A, Eyeberu A et al (2022) Precancerous cervical lesion among adult women with human immune deficiency virus on anti retroviral therapy at Saint Peter Specialized Hospital, Ethiopia: a hospital-based cross-sectional study. Front Oncol 12:910915
Begoihn M, Mathewos A, Aynalem A, Wondemagegnehu T, Moelle U, Gizaw M et al (2019) Cervical cancer in Ethiopia—predictors of advanced stage and prolonged time to diagnosis. Infect Agents Cancer 14(1):1–7
Dereje N, Addissie A, Worku A, Gebremariam A, Kantelhardt EJ, Assefa M et al (2021) Association between waiting time for radiotherapy initiation and disease progression among women with cervical cancer in Addis Ababa, Ethiopia. Int J Cancer 149(6):1284–1289
Zeleke S, Anley M, Kefale D, Wassihun B (2021) Factors associated with delayed diagnosis of cervical cancer in Tikur Anbesa specialized hospital, Ethiopia, 2019: cross-sectional study. Cancer Manag Res 13:579–585
Atnafu T, Daka DW, Debela TF, Ergiba MS (2021) Women’s satisfaction with cervical cancer screening services and associated factors in maternal health clinics of Jimma Town Public Health Facilities, Southwest Ethiopia. Cancer Manag Res 13:7685–7696
Dirar A, Mekonnen W, Berhanu Z (2022) The experiences of cervical cancer patients during follow-up care in Ethiopia: a qualitative study. Cancer Manag Res 14:2507–2518
Kebebew T, Mosalo A, Mavhandu-Mudzusi AH (2022) Caregivers’ satisfaction with cervical cancer care in Ethiopia. Support Care Cancer 30(9):7597–7603
Endale H, Mulugeta T, Habte T (2022) The socioeconomic impact of cervical cancer on patients in Ethiopia: evidence from Tikur Anbessa specialized hospital. Cancer Manag Res 14:1615–1625
Araya LT, Fenta TG, Sander B, Gebremariam GT, Gebretekle GB (2020) Health-related quality of life and associated factors among cervical cancer patients at Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia. Health Qual Life Outcomes 18(1):1–9
Hailu A, Mariam DH (2013) Patient side cost and its predictors for cervical cancer in Ethiopia: a cross sectional hospital based study. BMC Cancer 13:1–8
Deressa BT, Assefa M, Tafesse E, Kantelhardt EJ, Soldatovic I, Cihoric N et al (2021) Contemporary treatment patterns and survival of cervical cancer patients in Ethiopia. BMC Cancer 21(1):1–7
Wassie M, Argaw Z, Tsige Y, Abebe M, Kisa S (2019) Survival status and associated factors of death among cervical cancer patients attending at Tikur Anbesa Specialized Hospital, Addis Ababa, Ethiopia: a retrospective cohort study. BMC Cancer 19(1):1221
Wassie M, Fentie B (2021) Prevalence of late-stage presentation and associated factors of cervical cancer patients in Tikur Anbesa Specialized Hospital, Ethiopia: institutional based cross-sectional study. Infect Agents Cancer 16(1):30
Seifu B, Fikru C, Yilma D, Tessema F (2022) Predictors of time to death among cervical cancer patients at Tikur Anbesa specialized hospital from 2014 to 2019: a survival analysis. PLoS One 17(2):e0264369
Gashu C, Tasfa B, Alemu C, Kassa Y (2023) Assessing survival time of outpatients with cervical cancer: at the university of Gondar referral hospital using the Bayesian approach. BMC Womens Health 23(1):59
Aguade AE, Gashu C, Jegnaw T (2023) The trend of change in cervical tumor size and time to death of hospitalized patients in northwestern Ethiopia during 2018–2022: retrospective study design. Health Sci Rep 6(2):e1121
Mebratie AE, Moges NA, Meselu BT, Melesse MF (2022) Time to death from cervical cancer and predictors among cervical cancer patients in Felege Hiwot Comprehensive Specialized Hospital, North West Ethiopia: facility-based retrospective follow-up study. PLoS One 17(6):e0269576
Moelle U, Mathewos A, Aynalem A, Wondemagegnehu T, Yonas B, Begoihn M et al (2018) Cervical cancer in Ethiopia: the effect of adherence to radiotherapy on survival. Oncologist 23(9):1024–1032
Gizaw M, Addissie A, Getachew S, Ayele W, Mitiku I, Moelle U et al (2017) Cervical cancer patients presentation and survival in the only oncology referral hospital, Ethiopia: a retrospective cohort study. Infect Agents Cancer 12(1):1–7
Getaneh A, Tegene B, Belachew T (2021) Knowledge, attitude and practices on cervical cancer screening among undergraduate female students in University of Gondar, Northwest Ethiopia: an institution based cross sectional study. BMC Public Health 21(1):775
Wakwoya EB, Gemechu KS, Dasa TT (2020) Knowledge of cervical cancer and associated factors among women attending public health facilities in Eastern Ethiopia. Cancer Manag Res 12:10103–10111
Chali K, Oljira D, Sileshi T, Mekonnen T (2021) Knowledge on cervical cancer, attitude toward its screening, and associated factors among reproductive age women in Metu Town, Ilu Aba Bor, South West Ethiopia, 2018: community-based cross-sectional study. Cancer Rep (Hoboken) 4(5):e1382
Tekle T, Wolka E, Nega B, Kumma WP, Koyira MM (2020) Knowledge, attitude and practice towards cervical cancer screening among women and associated factors in hospitals of Wolaita Zone, Southern Ethiopia. Cancer Manag Res 12:993–1005
Bogale AL, Teklehaymanot T, Haidar Ali J, Kassie GM (2021) Knowledge, attitude and practice of cervical cancer screening among women infected with HIV in Africa: systematic review and meta-analysis. PLoS One 16(4):e0249960
Belete N, Tsige Y, Mellie H (2015) Willingness and acceptability of cervical cancer screening among women living with HIV/AIDS in Addis Ababa, Ethiopia: a cross sectional study. Gynecol Oncol Res Pract 2:6
Eshete M, Abdulwuhab Atta M, Yeshita HY (2020) Cervical cancer screening acceptance among women in Dabat District, Northwest Ethiopia, 2017: an institution-based cross-sectional study. Obstet Gynecol Int 2020:2805936
Ampofo AG, Boyes AW, Khumalo PG, Mackenzie L (2022) Improving knowledge, attitudes, and uptake of cervical cancer prevention among female students: a systematic review and meta-analysis of school-based health education. Gynecol Oncol 164:675–690
Ortenzi F, Marten R, Valentine NB, Kwamie A, Rasanathan K (2022) Whole of government and whole of society approaches: call for further research to improve population health and health equity. BMJ Spec J 7:e009972
Spayne J, Hesketh T (2021) Estimate of global human papillomavirus vaccination coverage: analysis of country-level indicators. BMJ Open 11(9):e052016
Dorji T, Nopsopon T, Tamang ST, Pongpirul K (2021) Human papillomavirus vaccination uptake in low-and middle-income countries: a meta-analysis. EClinicalMedicine 34:100836
Mavundza EJ, Iwu-Jaja CJ, Wiyeh AB, Gausi B, Abdullahi LH, Halle-Ekane G et al (2021) A systematic review of interventions to improve HPV vaccination coverage. Vaccines 9(7):687
Belay Y, Dheresa M, Sema A, Desalew A, Assefa N (2020) Cervical cancer screening utilization and associated factors among women aged 30 to 49 years in Dire Dawa, Eastern Ethiopia. Cancer Control 27(1):1073274820958701
Moyo S, Petersen Z, Jaca A, Zungu N, Takatshana S, Maseko G et al (2018) Barriers to uptake of cervical cancer screening services in low-and-middle-income countries: a systematic review. Indian J Cancer 55:318–326
Kassie AM, Abate BB, Kassaw MW, Aragie TG, Geleta BA, Shiferaw WS (2020) Impact of knowledge and attitude on the utilization rate of cervical cancer screening tests among Ethiopian women: a systematic review and meta-analysis. PLoS One 15(12):e0239927
Bruni L, Serrano B, Roura E, Alemany L, Cowan M, Herrero R et al (2022) Cervical cancer screening programmes and age-specific coverage estimates for 202 countries and territories worldwide: a review and synthetic analysis. Lancet Glob Health 10(8):e1115–e1127
Amado G, Weldegebreal F, Birhanu S, Dessie Y (2022) Cervical cancer screening practices and its associated factors among females of reproductive age in Durame town, Southern Ethiopia. PLoS One 17(12):e0279870
Tefera F, Mitiku I (2017) Uptake of cervical cancer screening and associated factors among 15–49-year-old women in Dessie Town, Northeast Ethiopia. J Cancer Educ 32(4):901–907
Mezei AK, Armstrong HL, Pedersen HN, Campos NG, Mitchell SM, Sekikubo M et al (2017) Cost-effectiveness of cervical cancer screening methods in low-and middle-income countries: a systematic review. Int J Cancer 141(3):437–446
Robbers GML, Bennett LR, Spagnoletti BRM, Wilopo SA (2021) Facilitators and barriers for the delivery and uptake of cervical cancer screening in Indonesia: a scoping review. Glob Health Action 14(1):1979280
Gutusa F, Roets L (2023) Early cervical cancer screening: the influence of culture and religion. Afr J Prim Health Care Fam Med 15(1):3776
Dareng EO, Jedy-Agba E, Bamisaye P, Isa Modibbo F, Oyeneyin LO, Adewole AS et al (2015) Influence of spirituality and modesty on acceptance of self-sampling for cervical cancer screening. PLoS One 10(11):e0141679
De Abreu CS (2015) How socio-cultural factors affect cervical cancer screening adherence and treatment in disadvantaged communities in the greater Cape Town. University of Cape Town, Cape Town
Padela AI, Peek M, Johnson-Agbakwu CE, Hosseinian Z, Curlin F (2014) Associations between religion-related factors and cervical cancer screening among Muslims in greater Chicago. J Low Genit Tract Dis 18(4):326
Medcalfe SK, Slade CP, Habegger W (2023) Religion as a social determinant of women’s cancer screening: evidence from state level data for policy and resource allocation. Am J Econ Sociol 82(3):263–279
Bayrami R, Taghipour A, Ebrahimipour H (2015) Personal and socio-cultural barriers to cervical cancer screening in Iran, patient and provider perceptions: a qualitative study. Asian Pac J Cancer Prev 16(9):3729–3734
Gebresilasie SF, Zegeye A (2022) Accuracy of VIA for the diagnosis of cervical cancer and associated factors among women attending cervical cancer screening at Hawassa university comprehensive specialized hospital, southern Ethiopia: Institutional based cross sectional study. Ann Med Surg (Lond) 84:104873
Hull R, Mbele M, Makhafola T, Hicks C, Wang SM, Reis RM et al (2020) Cervical cancer in low and middle-income countries. Oncol Lett 20(3):2058–2074
Zena D, Elfu B, Mulatu K (2021) Prevalence and associated factors of precancerous cervical lesions among women in Ethiopia: a systematic review and meta-analysis. Ethiop J Health Sci 31(1):189–200
Dau H, Trawin J, Nakisige C, Payne BA, Vidler M, Singer J et al (2023) The social and economic impacts of cervical cancer on women and children in low-and middle-income countries: a systematic review. Int J Gynecol Obstet 160(3):751–761
Download references
Authors did not receive any fund to publish this article.
Author information
Authors and affiliations.
School of Public Health, The University of Queensland, Brisbane, Australia
Aklilu Endalamaw & Yibeltal Assefa
College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia
Aklilu Endalamaw, Habtamu Alganeh & Muluken Azage
College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Asmamaw Atnafu, Adane Nigusie & Destaw Fetene Teshome
Centre for Applied Health Economics, School of Medicine, Griffith University, Brisbane, Australia
Daniel Erku
Menzies Health Institute Queensland, Griffith University, Brisbane, Australia
International Institute of Primary Health Care, Addis Ababa, Ethiopia
Eskinder Wolka & Anteneh Zewdie
You can also search for this author in PubMed Google Scholar
Contributions
AE and YA conceptualised the study design, retrieved relevant articles, screening and data extraction, analysed, interpreted the results, and drafted the manuscript. HA contributed to selection of articles and data extraction. MA, AA, DE and EW contributed to the research aim and manuscript draft, and critically revised the drafted manuscript. AN, AZ and DFT contributed to critically revised the drafted manuscript. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Aklilu Endalamaw .
Ethics declarations
Conflict of interest.
The authors declare no competing interests.
Ethical approval
As the study depend on publicly available literature, ethical approval did not be required.
Consent for publication
Not applicable.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (DOCX 32 KB)
Supplementary file2 (docx 17 kb), supplementary file3 (docx 17 kb), supplementary file4 (docx 27 kb), supplementary file5 (docx 21 kb), supplementary file6 (docx 16 kb), supplementary file7 (docx 33 kb), rights and permissions.
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Endalamaw, A., Alganeh, H., Azage, M. et al. Improving cervical cancer continuum of care towards elimination in Ethiopia: a scoping review. Cancer Causes Control 35 , 549–559 (2024). https://doi.org/10.1007/s10552-023-01813-9
Download citation
Received : 12 April 2023
Accepted : 06 October 2023
Published : 04 November 2023
Issue Date : March 2024
DOI : https://doi.org/10.1007/s10552-023-01813-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Cervical cancer
- Find a journal
- Publish with us
- Track your research
- History, Facts & Figures
- YSM Dean & Deputy Deans
- YSM Administration
- Department Chairs
- YSM Executive Group
- YSM Board of Permanent Officers
- FAC Documents
- Current FAC Members
- Appointments & Promotions Committees
- Ad Hoc Committees and Working Groups
- Chair Searches
- Leadership Searches
- Organization Charts
- Faculty Demographic Data
- Professionalism Reporting Data
- 2022 Diversity Engagement Survey
- State of the School Archive
- Faculty Climate Survey: YSM Results
- Strategic Planning
- Mission Statement & Process
- Beyond Sterling Hall
- COVID-19 Series Workshops
- Previous Workshops
- Departments & Centers
- Find People
- Biomedical Data Science
- Health Equity
- Inflammation
- Neuroscience
- Global Health
- Diabetes and Metabolism
- Policies & Procedures
- Media Relations
- A to Z YSM Lab Websites
- A-Z Faculty List
- A-Z Staff List
- A to Z Abbreviations
- Dept. Diversity Vice Chairs & Champions
- Dean’s Advisory Council on Lesbian, Gay, Bisexual, Transgender, Queer and Intersex Affairs Website
- Minority Organization for Retention and Expansion Website
- Office for Women in Medicine and Science
- Committee on the Status of Women in Medicine Website
- Director of Scientist Diversity and Inclusion
- Diversity Supplements
- Frequently Asked Questions
- Recruitment
- By Department & Program
- News & Events
- Executive Committee
- Aperture: Women in Medicine
- Self-Reflection
- Portraits of Strength
- Mindful: Mental Health Through Art
- Event Photo Galleries
- Additional Support
- MD-PhD Program
- PA Online Program
- Joint MD Programs
- How to Apply
- Advanced Health Sciences Research
- Clinical Informatics & Data Science
- Clinical Investigation
- Medical Education
- Visiting Student Programs
- Special Programs & Student Opportunities
- Residency & Fellowship Programs
- Center for Med Ed
- Organizational Chart
- Committee Procedural Info (Login Required)
- Faculty Affairs Department Teams
- Recent Appointments & Promotions
- Academic Clinician Track
- Clinician Educator-Scholar Track
- Clinican-Scientist Track
- Investigator Track
- Traditional Track
- Research Ranks
- Instructor/Lecturer
- Social Work Ranks
- Voluntary Ranks
- Adjunct Ranks
- Other Appt Types
- Appointments
- Reappointments
- Transfer of Track
- Term Extensions
- Timeline for A&P Processes
- Interfolio Faculty Search
- Interfolio A&P Processes
- Yale CV Part 1 (CV1)
- Yale CV Part 2 (CV2)
- Samples of Scholarship
- Teaching Evaluations
- Letters of Evaluation
- Dept A&P Narrative
- A&P Voting
- Faculty Affairs Staff Pages
- OAPD Faculty Workshops
- Leadership & Development Seminars
- List of Faculty Mentors
- Incoming Faculty Orientation
- Faculty Onboarding
- Past YSM Award Recipients
- Past PA Award Recipients
- Past YM Award Recipients
- International Award Recipients
- Nominations Calendar
- OAPD Newsletter
- Fostering a Shared Vision of Professionalism
- Academic Integrity
- Addressing Professionalism Concerns
- Consultation Support for Chairs & Section Chiefs
- Policies & Codes of Conduct
- Health & Well-being
- First Fridays
- Fund for Physician-Scientist Mentorship
- Grant Library
- Grant Writing Course
- Mock Study Section
- Research Paper Writing
- Funding Opportunities
- Join Our Voluntary Faculty
- Faculty Resources
- Research by Keyword
- Research by Department
- Research by Global Location
- Translational Research
- Research Cores & Services
- Program for the Promotion of Interdisciplinary Team Science (POINTS)
- CEnR Steering Committee
- Experiential Learning Subcommittee
- Goals & Objectives
- Embryonic Stem Cell Research Oversight
- COVID-19 Vaccinations in CT
- COVID-19 in Connecticut Schools
- Connecticut Towns COVID-19 Impact Dashboard
- Connecticut Town 14-Day Cases Time Lapse
- CT Correctional Facilities with COVID Cases Dashboard
- Connecticut COVID Presence Map
- CT Nursing Homes with COVID-19 Cases
- U.S. COVID Presence Map
- COVID-19 Case Density by US County
- Global Cases Dashboard
- Time-Lapse of Global Spread
- US Racial and Ethnic Disparities in COVID-19 Mortality
- Childcare Survey and Data Display
- Risk of Complications Conditional on COVID-19 Infection
- Travel Time to COVID Testing Sites in Connecticut
- Travel Time to COVID Testing Sites in the US
- Project Team
- Issues List
- Print Magazine PDFs
- Print Newsletter PDFs
- YSM Events Newsletter
- Social Media
- Patient Care
INFORMATION FOR
- Residents & Fellows
- Researchers
Genetic Analysis of Rare, Often Deadly Cervical Cancer Uncovers Potential Treatments
Largest translational study seeking novel treatments specifically for neuroendocrine tumors of the cervix (netc)., microscopic image of cervical cancer.
This was the largest translational study seeking novel treatments specifically for neuroendocrine tumors of the cervix (NETc).
An ambitious study of patients from around the world with rare neuroendocrine tumors of the cervix (NETc) set out to uncover potential treatments by understanding the molecular basis of the aggressive disease. Since the average survival for patients diagnosed with NETc is less than two years, effective treatments are needed.
Yale Cancer Center (YCC) researchers at Yale School of Medicine (YSM) analyzed the genetic landscape of 66 tumors, the largest series of cervical NET ever reported in scientific literature. They used cutting-edge techniques (whole-exome and RNA-Seq analysis) to sequence all the genes from the tumors and identified the mutations that are crucial for these tumors to grow and endure cancer treatment.
The study, conducted through international collaboration with research groups in Italy, Norway, South Korea, and the United States, revealed atypical genes and pathways that indicate NET patients could benefit from precision medicine. Researchers say the findings better define the genetic landscape of NETc and suggest that a large subset of these highly aggressive malignancies might respond to existing targeted therapies.
The study was published April 15 in Proceedings of the National Academy of Sciences .
“Our findings have important implications for the development of novel therapies since NETc are currently treated with chemotherapy regimens used for patients with lung cancer,” said senior author Alessandro Santin, MD , co-chief of the division of gynecologic oncology at YCC and a professor of obstetrics, gynecology & reproductive sciences at YSM. “Our genetic data suggest that regimens used for the most common types of cervical cancer in combination with immunotherapies may represent a better choice.”
Stefania Bellone, PhD , first author of the study and associate research scientist in the Department of Obstetrics, Gynecology & Reproductive Sciences at YSM, said that the genetic sequencing of tumors with both adenocarcinoma and neuroendocrine elements found for the first time that the neuroendocrine part of the tumor comes from the same type of cell that leads to the adenocarcinoma, meaning they each have similar genetic mutations typical of epithelial cancer.
The study team sequenced tumor genes from 64 patients affected with NETc, including two patients with NETc tumors mixed with adenocarcinoma cells, cancer cells that form in glands that line certain organs. Using two fully sequenced patient-derived xenografts (PDX) — in which patients’ cancer cells were implanted in mice — the researchers identified mutations that were crucial for the tumors to grow and survive treatment. The team also studied genes that were not mutated but were amplified in the tumors to give them a growth advantage over normal tissues.
The findings showed many genes had repeated mutations and some had higher levels of certain genetic changes than others. Tumors with a higher number of mutations are potentially more sensitive to immunotherapy.
Corresponding author Joseph Schlessinger, PhD , the William H. Prusoff Professor of Pharmacology at YSM, said that creating two PDX models, each with their own mutation profile, allowed testing of each to determine if they could predict drug responses in living organisms. The approach held promise for tailoring cancer treatments to individual patients.
Other Yale authors on the study include Blair McNamara , Michelle Greenman , Levent Mutlu , Cem Demirkiran , Tobias Max Philipp Hartwich , Yang Yang-Hartwich , Natalia Buza , Pei Hui , Gary Altwerger , Gloria Huang , Vaagn Andikyan , Mitchell Clark , Elena Ratner , Masoud Azodi , Peter E. Schwartz , and Ludmil B. Alexandrov
Featured in this article
- Alessandro Santin, MD
- Stefania Bellone, PhD
- Joseph Schlessinger, PhD
- Blair Colette McNamara, MD
- Michelle Greenman
- Levent Mutlu, MD
- Cem Demirkiran, MD
- Tobias Hartwich, PhD
- Yang Yang, PhD
- Natalia Buza, MD
- Pei Hui, PhD, MD
- Gary Altwerger, MD
- Gloria Huang, MD, FACOG
- Vaagn Andikyan, MD
- Mitchell Clark, MD, MPH
- Peter Schwartz, MD
- Elena Ratner, MD, MBA
- Ludmil B. Alexandrov, PhD
- Masoud Azodi, MD

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Cancers (Basel)
Candidate Genes and Pathways in Cervical Cancer: A Systematic Review and Integrated Bioinformatic Analysis
Marjanu hikmah elias.
1 Department of Basic Medical Sciences I, Faculty of Medicine & Health Sciences, Universiti Sains Islam Malaysia, Nilai 71800, Malaysia
2 Department of Human & Clinical Anatomy, College of Medicine and Health Sciences, Sultan Qaboos University, Muscat 123, Oman
Nazefah Abdul Hamid
Associated data, simple summary.
Cervical cancer is the fourth most common cancer among women worldwide. Although many recommendations on the screening, diagnosis, and treatment of cervical cancer have been established, no comprehensive molecular mechanism for cervical cancer has been determined. Hence, this systematic review and integrated bioinformatic analysis provides new insight into the key genes and pathways involved in the pathogenesis of cervical cancer and, thus, can be beneficial for developing better screening and treatment strategies for cervical cancer.
Cervical cancer is the leading cause of cancer-related death among women in developing countries. However, no comprehensive molecular mechanism for cervical cancer has been established, as many studies were small-cohort studies conducted with small sample sizes. A thorough literature search was performed using the PubMed, Scopus, EBSCOhost, and Science Direct databases. Medical Subject Heading (MeSH) terms such as “Uterine Cervical Neoplasms” and “gene expression” were used as the keywords in all fields. A total of 4027 studies were retrieved, and only clinical studies, which used the microarray method to identify differentially expressed genes (DEGs) in the cervical tissue of cervical cancer patients, were selected. Following the screening, 6 studies were selected and 1128 DEGs were extracted from the data. Sixty-two differentially expressed genes from at least two studies were selected for further analysis by DAVID, STRING, and Cytoscape software. In cervical cancer pathogenesis, three significant clusters with high intermolecular interactions from the Protein–Protein Interaction (PPI) network complex revealed three major molecular mechanisms, including cell signaling, cell cycle, and cell differentiation. Subsequently, eight genes were chosen as the candidate genes based on their involvement in the relevant gene ontology (GO) and their interaction with other genes in the PPI network through undirected first neighbor nodes. The present systematic review improves our understanding of the molecular mechanism of cervical cancer and the proposed genes that can be used to expand the biomarker panel in the screening for cervical cancer. The targeted genes may be beneficial for the development of better treatment strategies.
1. Introduction
Cervical cancer is the fourth most common cancer in women worldwide, with an estimated incidence of 570,000 and 311,000 related deaths in 2018 [ 1 ]. Although the incidence of cervical cancer has declined in the United States, it remains the leading cause of cancer-related death in developing countries [ 2 ]. Thus, many recommendations on the screening, diagnosis, and treatment of cervical cancer have been established [ 2 , 3 , 4 ]. A recent recommendation on multiple-agent chemotherapy regimens that include targeted therapies and immunotherapy regimens in combination with the existing first- and second-line treatment options has improved the outcomes in some cervical cancer patients [ 3 ]. However, cervical cancer is a multifactorial disease that involves complex pathophysiology and molecular pathogenesis. Thus, further studies are still crucial to providing comprehensive information on the mechanism of cervical cancer pathogenesis that is critical in developing better screening, diagnosis, and treatment of cervical cancer.
Several molecular mechanisms have been proposed for cervical cancer involving genomic variations [ 5 ], regulation of mRNA expression [ 6 ], and epigenetic changes [ 7 ]. Various pathways have been identified to be involved in cervical cancer through the regulation of gene expression including MAPK, mTOR, PI3K-Akt , the Ras signaling pathway, immune response, inflammation, DNA synthesis, cell proliferation, and many others [ 8 , 9 ]. Identifying the DEGs and their key pathways and functions can improve our understanding of the molecular mechanisms that occur in cervical cancer pathogenesis. Therefore, many studies on gene-expression profiling have been conducted on cervical cancer patients, and hundreds of DEGs have been identified. From these studies, many potential biomarkers have been proposed, such as FBL1 , ANT3 [ 10 ], RBBP6 [ 11 ], TMEM45A , SERPINB5, p16INK4A [ 12 ], and many more. However, these studies only focused on a single cohort from different populations, with a small sample size, and employed different methods to identify the DEGs. Thus, these individual results could not robustly represent the pathogenesis of cervical cancer due to various biases. Hence, this systematic review was performed to identify the pattern of gene expression, functions, interactions, and critical pathways with minimal bias in the cervical tissue of cervical cancer patients across populations via integrated bioinformatic analysis.
2. Materials and Methods
2.1. search strategy.
The systematic review was conducted according to the PRISMA guidelines. This systematic review was registered with OpenScience Framework. A comprehensive literature search was carried out using the PubMed, Scopus, EBSCOhost, and Science Direct databases. Related research papers published up to 15 February 2022 were identified. Medical Subject Heading (MeSH) terms such as “uterine cervical neoplasms” and “gene expression” were used as the keywords in all fields. Synonyms for the keywords were generated through MeSH terms from the Cochrane Library. Additional text terms were found by assessing the collected review articles. The search strategy involved a combination (“AND”) of the following sets of keywords: (1) “uterine cervical neoplasms” OR “cervical intraepithelial neoplasia” OR “cervical cancer” and (2) “gene expression.” Additional references were identified from the bibliographies of the retrieved studies.
2.2. Inclusion Criteria
Case–control, cross-sectional, and prospective observational studies with abstracts investigating the DEGs in the cervical tissue of cervical cancer patients were included. Only clinical studies using the microarray method to identify differentially expressed genes (DEGs) in the cervical tissue of cervical cancer patients were included to ensure the homogeneity of the data. Studies reporting a list of DEGs were included in this systematic review.
2.3. Exclusion Criteria
Publications without primary data, such as editorials, case reports, conference proceedings, and narrative review articles, were excluded. In silico, in vitro, and in vivo studies were excluded. Intervention studies for cervical cancer treatment and those using blood and non-cervical tissue samples were excluded. Studies that utilized other gene-expression methods, such as quantitative PCR, were not selected to avoid bias in gene selection. Next-Generation Sequencing (NGS) studies were excluded to avoid allele expression biases. Studies that did not include the list of DEGs in their report, supplementary materials , or links to any other sources were also excluded.
2.4. Screening of Articles for Eligibility
Three phases of screening were performed on articles recovered from all resources. Duplicates were removed, and all articles with non-relevant titles were excluded in the first phase. The abstracts of the remaining articles were examined, and articles that did not meet the inclusion criteria were excluded from the second phase. Finally, the full texts of the remaining articles were reviewed thoroughly. Systematic reviews; meta-analyses; in vitro, in vivo, and in silico articles; and articles that did not meet the inclusion criteria were excluded in this third phase. All the authors were involved in the screening, selection, and data extraction phases. Figure 1 shows the PRISMA flow diagram summarizing the article-sorting process, and the reasons for article elimination.

PRISMA flow diagram for studies’ selection in this systematic review.
2.5. Data Extraction
Data were extracted from the studies that fulfilled the inclusion criteria. All the authors participated in extracting the data. A data collection form was used to standardize the data collection, and all data extraction was performed independently. Any disagreements were discussed, decisions were made based on the majority consensus, and records of reasons for rejection were kept. The collected data are as follows: (1) author’s name, (2) article title, (3) study design, (4) sample size, (5) type of sample, (6) gene-expression method, (7) list of DEGs, and (8) conclusion.
2.6. Study Quality
The study quality of each paper was evaluated independently by NAH and MHE using the Joanna Briggs Institute critical appraisal tools [ 13 ]. The results of the quality of the study were validated by MHE and NAH. An overall score of less than 50% was used to rate a paper as a low-quality (high risk of bias) paper. If the overall score was 50–69%, it was rated as a moderate-quality (moderate risk of bias) paper, and if the overall score was more than 69%, it was rated as a high-quality (low risk of bias) paper.
2.7. Venn Diagram Analysis
All the DEGs were extracted and listed according to the studies. Then, a Venn diagram analysis was carried out using Bioinformatics & Evolutionary Genomics software [ 14 ]. The Venn diagram analysis was performed to identify the common DEGs between studies. Differentially expressed genes in at least two studies were selected for further analysis.
2.8. Protein–Protein Interaction (PPI) Network, Clustering, and Visualization
All selected DEGs from the Venn diagram analysis were pooled and analyzed through a PPI functional-enrichment analysis via STRING software (version 11.5, STRING Consortium 2022, Zurich, Switzerland, https://string-db.org/ accessed on 28 October 2022) to identify the PPI network [ 15 ]. The results from STRING were exported into Cytoscape software (version 3.8.0, Cytoscape Consortium, San Diego, CA, USA, http://www.cytoscape.org/ , accessed on 4 November 2022) to visualize the molecular interaction networks and to integrate the gene-expression profiles of the DEGs [ 16 ]. A module analysis of the target network and protein clustering were performed using the Cytoscape MCODE plug-in (degree cut-off = 2, node score cut-off = 0.2, node density cut-off = 0.1, K-score = 2, and max depth = 100). The significantly enriched gene ontology was identified by analyzing the list of genes in each cluster using DAVID software (version 2021, DAVID Bioinformatic team, Frederick, MD, USA).
2.9. Gene Ontology (GO) and Pathway Enrichment Analysis
All the genes in each cluster were analyzed using the Database for Annotation, Visualization, and Integrated Discovery (DAVID) to discover the gene ontology that exhibited significant functional annotation enrichment related to cervical cancer pathogenesis [ 17 ]. Finally, the Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway was utilized to expose the involvement of genes in the pathway related to cervical cancer [ 18 ].
The four databases generated 4027 potentially relevant studies from the keywords. Based on the title, 307 duplicates were removed, and the abstracts of the other 3720 were screened. Upon screening the abstracts, 3681 papers were excluded. The full text of the other 24 papers was then retrieved. After a thorough review of the full text, 18 articles that did not meet the inclusion and exclusion criteria were excluded. Finally, six studies were selected for this systematic review. These six studies were published between the years 2006 and 2021. Prevention of sampling bias was assured through homogenized sampling by adhering strictly to the specific inclusion and exclusion criteria. Only studies that performed microarray analyses were chosen, and the sample size was between 2 and 25. Table 1 shows a summary of the characteristics of the included studies.
Summary of the characteristics of the included studies.
3.1. Patient Recruitment and Sample Collection Details
Sample collection was described in all studies. Kim et al. (2013), Miyatake et al. (2007), and Wong et al. (2006) stated that the staging of cervical cancer was carried out according to the International Federation of Gynaecology and Obstetrics (FIGO) criteria [ 20 , 22 , 24 ]. However, not all studies elaborated on the demographic profile of their patients. While the other five studies collected biopsies, Rajkumar et al. (2011) collected the archive-extracted total RNA from the biobank [ 21 ]. Normal cervical tissue biopsies were collected from women who underwent hysterectomy for other gynecological-related problems [ 19 , 21 , 24 ], from uterine leiomyoma patients [ 20 ], and from normal tissue adjacent to cervical squamous epithelia [ 22 , 23 ].
3.2. Study Quality
A detailed quality assessment of the included studies is listed in Supplementary Table S1 . The included studies comprised four high-quality (low risk of bias) studies and two moderate-quality (moderate risk of bias) studies.
3.3. Identification of DEGs in Cervical Cancer
After removing duplicates, 1128 DEGs were extracted from all the selected studies. In the studies by Annapurna et al. (2021), Kim et al. (2013), Rajkumar et al. (2011), Miyatake et al. (2007), and Wong et al. (2006), only genes with an expression level of more than two or less than a negative two-fold change are identified as DEGs [ 19 , 20 , 21 , 22 , 24 ]. However, in the study by Gius et al. (2007), instead of using the fold change as a parameter to select DEGs, this study uses the calculated false discovery rate [ 23 ]. A list of 104, 409, 66, 22, 536, and 102 DEGs were reported in Annapurna et al. (2021), Kim et al. (2013), Rajkumar et al. (2011), Miyatake et al. (2007), Gius et al. (2007), and Wong et al. (2006), respectively [ 19 , 20 , 21 , 22 , 23 , 24 ].
3.4. Common DEGs among the Studies Identified via Venn Diagram Analysis
The common DEGs between studies were identified, in which CDH3 and CDKN2A were differentially expressed in four studies (Annapurna et al., 2021; Gius et al., 2007; Rajkumar et al., 2011; Wong et al., 2006) [ 19 , 21 , 23 , 24 ]. Four other genes ( BST2, PLSCR1, SPINK5, PLOD2 ) were common in three studies, and sixty-two genes were commonly expressed in two studies. Figure 2 shows the Venn diagram result for the DEGs from all the included studies. All 68 genes differentially expressed in at least two studies ( Supplementary Table S2 ) were selected for further analysis.

Venn diagram of the DEGs from all the selected studies.
3.5. Identification of Key Candidate Genes and Pathways via Protein–Protein Interaction (PPI) Network and Modular Analysis
Sixty-eight proteins from the selected DEGs were filtered into a PPI network complex containing 68 nodes and 181 edges with a PPI enrichment p -value of <1 × 10 −16 and an average local clustering coefficient of 0.602. The network’s data were transferred from STRING to Cytoscape software to visualize the molecular interaction networks. By utilizing the Molecular Complex Detection Algorithm (MCODE), three significant modules from the PPI network complex were discovered. Figure 3 shows the three significant clusters created from the PPI network complex generated from the DEGs in cervical cancer patients. The functional annotation clustering shows that cluster 1 comprises 20 nodes and 58 edges (score = 6.105), while cluster 2 consists of 7 nodes and 13 edges (score = 4.33), and cluster 3 consists of 4 nodes and 6 edges (score = 4).

PPI network of the DEGs collected from the selected studies.
3.6. Gene Ontology (GO) and Pathway Enrichment Analysis of the Identified Clusters
The GO and pathway enrichment analyses showed that the DEGs in cluster 1 were primarily located in the nucleoplasm and cytosol. These DEGs in cluster 1 involve the cell cycle and regulation of transcription. Their molecular functions include protein binding, DNA binding, ATP binding, and transcription factor binding. The DEGs in cluster 2 are primarily located in the cytoplasm and regulate cell adhesion, migration, and inflammatory and immune responses. The molecular function of DEGs in cluster 2 includes extracellular matrix binding, cytokine activity, and fibronectin binding.
The DEGs in cluster 3 were mainly situated in the cytosol and cornified envelope. These DEGs are involved in protein heterotetramerization, peptide cross-linking, and epithelial cell differentiation. The molecular function of DEGs in cluster 3 includes structural constituents of the epidermis. Table 2 summarizes the functional annotation clustering of the DEGs.
Functional annotation clustering of the DEGs with highlighted candidate genes.
3.7. Selection of Candidate Genes in Cervical Cancer Pathogenesis
From the PPI network and the functional annotation clustering, eight genes were chosen as the candidate genes based on their involvement in the relevant GO and their interaction with other genes in the PPI network through undirected first neighbor nodes ( Figure 4 ). The candidate genes include CDNK2A, VEGFA, PTGS2, MCM2, MCM4, MCM6, KRT1 , and KRT10 . From the analysis, CDNK2A, VEGFA , and PTGS2 interacted closely. Meanwhile, the MCM and KRT families interact less with other clusters. Further details were extracted for all the candidate genes. Their expression levels in cervical cancer samples and functional annotation of each gene set are shown in Table 3 .

Protein interaction through undirected first neighbor of the candidate genes (highlighted in yellow) from cluster 1: ( a ) CDKN2A , ( b ) VEGFA , ( c ) PTGS2 , ( d ) MCM family, and ( e ) KRT family.
The expression regulation of candidate genes and their functional annotations.
4. Discussion
Understanding the comprehensive molecular mechanism of cervical cancer pathogenesis is crucial for developing better screening, management, and treatment for cervical cancer patients. Thus, many gene-expression studies on cervical cancer via various methods have been reported [ 9 , 25 , 26 ]. This systematic review comprehensively explored the contribution of gene expression and interaction in cervical cancer. From the six selected studies that reported on the DEGs in cervical samples of cervical cancer patients, 68 genes were differentially expressed in at least two studies. The PPI network and modular analysis revealed three significant clusters. All clusters showed high node connection and interaction, in which cluster 1 comprised 20 nodes and 58 edges, cluster 2 consisted of 7 nodes and 13 edges, and cluster 3 consisted of 4 nodes and 6 edges.
From the functional annotation clustering analysis, the primary molecular mechanism in cervical cancer is divided into three main mechanisms according to the clusters. The first mechanism, which includes the DEGs in cluster 1, is primarily involved in the cell cycle pathway and specifically in regulating the transcription process via ATP binding, single-stranded DNA binding, and transcription factor binding. The second mechanism, which includes the DEGs in cluster 2, is mainly involved in cell signaling that regulates cell proliferation, adhesion, and migration in response to infection and inflammation. The third mechanism, which includes the DEGs in cluster 3, mainly involves cell differentiation via the regulation of the keratin filament network through protein heterotetramerization.
The individual genes in each cluster were further analyzed, and seven candidate genes were selected; these were CDKN2A, VEGFA, PTGS2, MCM2, MCM4, MCM6, KRT1, and KRT10 . The CDKN2A protein is located in the nucleus and cytosol in cells (GO:0005634; GO:0005829) and is highly expressed in fat, testis, and adrenal tissue [ 27 ]. In cervical tissue, the expression of CDKN2A is typically low, but higher expression (6-fold to 342-fold change) was reported in cervical cancer tissue in four of the selected studies in this systematic review [ 19 , 21 , 23 , 24 ]. However, this finding is contradictory to an in vitro study by Luan et al. (2021) that reported on the low expression of CDKN2A in the cervical cancer cell lines and that the overexpression of CDKN2A inhibits cell proliferation and invasion of cervical cancer cells by arresting the cell cycle in the G1 phase [ 28 ]. Another contradictory finding was reported in an epigenetics study, in which the cervical cancer group showed significantly higher CDKN2A methylation than the control group [ 29 ], suggesting a low CDKN2A expression level in cervical cancer. Based on the significant interactions of CDKN2A with transcription factors, signaling molecules, and miRNAs, this gene has been proposed as a biomarker for cervical cancer prognosis [ 30 ]. Thus, due to the significantly promising role of CDKN2A in cervical cancer, further studies are crucial to address this conflicting finding.
The VEGFA protein is located in the cytoplasm of a cell and is highly expressed in thyroid, prostate, lung, and endometrium tissues [ 27 ]. In normal cervical tissue, the expression of VEGFA and its isoform ( VEGF165 ) is low but is upregulated in cervical cancer tissue [ 24 , 31 ]. VEGFA expression impacts cervical cancer cells’ apoptosis, proliferation, migration, and invasion [ 32 ]. Thus, the inhibition of VEGFA expression could lead to the inhibition of cell migration and invasive motility in cervical cancer cells [ 33 ] while the PTGS2 ( COX2 ) protein, located in the cytoplasm, is downregulated in cervical cancer tissue [ 20 , 22 ]. However, the overexpression of PTGS2 has been associated with a poor prognosis and resistance to cytotoxic therapy [ 34 ]. Several signaling mechanisms for regulating PTGS2 in cervical cancer have been validated, including the EGF and nuclear factor κB (NF-κB) pathways [ 35 ], and PAR2 through an EGFR-dependent mechanism [ 34 ].
MCM2, MCM4 , and MCM6 are from the minichromosome maintenance complex (MCM) protein family, which are essential components of the pre-replicative complex for the initiation of DNA replication and cell division [ 36 ]. In cervical cancer, MCM2 [ 24 ] and MCM6 are upregulated while MCM4 is downregulated [ 20 ]. However, the higher expression of MCM2, MCM4 , and MCM6 is significantly associated with favorable overall survival in cervical cancer patients [ 37 ].
KRT1 and KRT10 are from the cytokeratin gene family, which is highly expressed in the upper layer of the epidermis and the endothelial cells [ 38 ]. In cervical cancer, KRT1 (type II; “acidic” keratin) and KRT10 (type I; “basic” keratin) are upregulated in cervical cancer [ 21 ]. Thus, it is suggested that KRT1 and KRT10 are involved in the proliferation of cervical keratinocytes in cervical cancer.
Unlike the MCM family and KRT family, which interact closely within the cluster, CDKN2A, VEGFA , and PTGS2 show broader interactions when incorporating proteins from other clusters. Interestingly, the signal transducer and activator of transcription 1 ( STAT1 ) is found to interact with these three genes closely. STAT1 is a tumor suppressor gene that plays an essential role in apoptotic and anti-apoptotic signaling [ 39 ]. From the functional annotation analysis, CDKN2A , VEGFA, PTGS2 , and STAT1 were involved in cancer pathways (hsa05200; KEGG pathway). The combination and interaction of these genes in cancer pathogenesis cover the major signaling pathways in cancer, such as proliferation, angiogenesis, cell cycle, and apoptosis pathways.
Major signaling pathways in proliferation, cell cycle, migration, apoptosis, and DNA repair are primarily involved in cancer development [ 40 , 41 , 42 ]. The phosphatidylinositol 3-kinase/protein kinase B/mammalian target of rapamycin (PI3K/AKT/mTOR) signaling pathway involved in cell proliferation, survival, invasion, migration, apoptosis, glucose metabolism, and DNA repair is associated with breast cancer pathogenesis [ 43 ]. Meanwhile, the JAK/STAT pathway, PI3K/Akt/mTOR pathway, Ras/Raf/MAPK pathway, and Wnt/β-catenin pathway contributed to hepatocellular carcinoma by regulating the cell growth, differentiation, apoptosis, and survival [ 44 ].
Besides the major signaling pathways usually exhibited by most cancers, cervical cancer also exhibits its unique pathways. From the functional annotation clustering performed, cervical cancer was also found to involve pathways related to infections such as human papillomavirus infection (hsa05165), human cytomegalovirus infection (hsa05163), human T-cell leukemia virus 1 infection (hsa05166), and staphylococcus aureus infection (hsa05150). Pathways that respond to infection such as NOD-like receptor-signaling pathway (hsa04621) and Toll-like receptor-signaling pathway (hsa04620) are also involved in cervical cancer.
The strength of this systematic review is that it includes studies from various cohorts and populations. Thus, a more comprehensive molecular mechanism for cervical cancer with reduced effects of genetic variations between populations can be identified. The homogeneity and bias reduction of the data were assured by only incorporating the DEGs from the microarray result. The integrated bioinformatic analysis of the DEGs pooled from the systematic review helps to better interpret the genes’ function and involvement in the molecular mechanism of cervical cancer.
Nevertheless, the main limitation of this systematic review is the incomplete listing of differentially expressed genes in some of the studies and the various statistical analyses used by the included studies in identifying the DEGs. However, the homogeneity of the data was established by adhering to the strict inclusion criteria and by selecting only DEGs detected by microarray. This systematic review added new insight into the molecular mechanism of cervical cancer. It will be beneficial to elucidate further downstream mechanisms of the DEGs by using RNA interference or gene knockdown strategies.
5. Conclusions
The molecular interactions in the cervical tissue of cervical cancer patients required extensive investigation to identify a comprehensive molecular mechanism in cervical cancer pathogenesis. The integrated bioinformatic analysis from this systematic review reveals three major molecular mechanisms involved in cervical cancer pathogenesis: cell cycle, cell differentiation, and infection. CDKN2A, VEGFA, PTGS2, MCM2, MCM4, MCM6, KRT1, KRT10 , and STAT1 were identified as key genes that regulate cervical cancer pathogenesis and progression. These genes can be utilized to develop a biomarker panel for screening cervical cancer and can become targeted genes for developing better treatment strategies for cervical cancer.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/cancers15030853/s1 , Table S1: Quality assessment of the studies included in the systematic review; Table S2: The common differentially expressed genes in at least two studies.
Funding Statement
This research was funded by the Ministry of Higher Education, Malaysia under Fundamental Research Grant Scheme (FRGS/1/2012/SSK01/USIM/03/1; FRGS-PSK-32-50812) and USIM Internal Grant Scheme (PPPI/FPSK/0118/051000/15418).
Author Contributions
Conceptualization: M.H.E. and N.A.H.; Analysis: M.H.E. and N.A.H.; Writing: M.H.E., N.A.H. and S.D.; Editing: M.H.E., N.A.H. and S.D. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors have no competing interests to declare that are relevant to the content of this article. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
Community-Based Health Education on Cervical Cancer Essay
Introduction.
Community-based health education boosts the knowledge of women on cervical cancer, its signs, and symptoms, and improves their cervical cancer treatment uptake (Kolander et al., 2013). Through awareness, women will be able to understand the life of the diseases and the control measures that should be put in place to eradicate the infection. Women who have prior knowledge of cervical cancer, tend to take cervical screening services frequently as compared to those without knowledge of the disease.
The life expectancy of women typically exceeds that of men worldwide. In 46 nations in 2011, women’s life expectancy at birth exceeded 80 years, however, in the WHO African Region, it was just 58 years (Fouly & Hassen, 2020). Boys are much less likely than girls to experience sexual abuse.
Adolescent females die most frequently from automobile accidents in high- and upper-middle-income nations. The estimated 287 000 maternal fatalities per year, or nearly all (99%), take place in underdeveloped nations (Fouly & Hassen, 2020).
Maternal Health
The health of women throughout pregnancy, delivery, and the postpartum period is referred to as maternal health. To ensure that pregnant women achieve their maximum potential for health and well-being while maintaining the proper health of the fetus, each stage should be enjoyable. Despite significant advancement over the past 20 years, 30 000 women died during or after pregnancy and delivery in 2017. This amount is just too high (Fouly & Hassen, 2020).
The elimination of unnecessary maternal deaths must continue to be a key priority for the world (Penson, 2018). However, merely making it through pregnancy and delivery cannot serve as a benchmark for effective maternal health care.
Cervical Cancer
When cancer starts at the cervix it is referred to as cervical cancer. The cervix extends and connects the birth canal to the uterus (upper part of the womb). Every woman is at a risk of getting cancer of the cervix and it normally occurs in women at the age of above thirty years.
The majority of women die from the disease as a result of ignorance and poor screening process at cancer centers. The main cause of cancer in women is prolonged infection with some types of HPV (Fouly & Hassen, 2020).
Risk Factors of Cervical Cancer
The majority of cancers occur in people without any recognized risk factors, even though doctors have a notion of what may enhance your chance of developing cancer. Some elements that are known to raise your risk of cancer include lack of regular cervical screening, age, weird sexual behaviors, getting into early marriage, and having multiple sexual partners (Kolander et al., 2013). It is well-recognized that several lifestyle decisions raise your chance of developing cancer.
The cervical cancer mortality rate is high in women. The American cancer society projected that by 2025, there will be more than 2 million women suffering from cancer in the United States of America (Fouly & Hassen, 2020). Most women who are suffering from this disease are from developing countries where the cost of living is high and there are poor health care services. The relevant health body states could assist in reducing the rate of getting cervix cancer by offering regular screening and providing early treatment on time (Penson, 2018).
Causes of Cervical Cancer
Scientists have discovered that there is no single cause of cervical cancer. They believe that the interaction of several factors together caused cancer cells. The factors causing cervical cancer can be environmental, genetic, or at times caused by the genetic constitutional characteristics of a person. Additionally, HPV is claimed to be the major cause of cervical cancer. HPV has been classified into three district types by the World Health Organization and these include; Carcinogenic (HPV types 16 and 18), Probably carcinogenic (HPV types 31 and 33), and possibly carcinogenic (other HPV types excerpt 6 and 11) (Penson, 2018).
From the cancer tests and screenings done, it was found that no. 16 is prevalent among all types of cancer. Out of the total samples collected, approximately of 82% tested with type 16 (Fouly & Hassen, 2020). This kind of cancer affects the entire birth canal unlike type 18 that only affects the endocervical gland. Another type of cervical cancer that is very common after type 16 is 35 (Penson, 2018).
Prevention of Cervical Cancer
Smoking is associated with more cancers than simply lung cancer. You can lower your future chance of developing cancer by giving up now. The sun’s harmful ultraviolet (UV) radiation might raise one’s chance of developing skin cancer. Reduce your exposure to the sun by seeking out shade, using sunscreen, or donning protective gear. Obesity or being overweight may raise your chance of developing cancer (Fouly & Hassen, 2020). By combining a nutritious diet with regular exercise, work to reach and maintain a healthy weight.
Encouraging the Target Audience to Take Action
Presently, it is vital to promote the importance of awareness regarding the issue of cervical cancer in the target population. Specifically, it is necessary to empower women and girls to seek active health education and support from healthcare experts. Thus, the importance of regular tests, including pap smears, must be explained to the specified demographic. Specifically, healthcare experts and nurses must prompt active communication between women and healthcare practitioners, gynecologists, and endocrinologists. Thus, active education must be promoted. Specifically, women and girls must be provided with core information about the means of preventing cancer and the strategies for identifying the relevant risk and threats at the earliest stage possible. Thus, fatal outcomes in women can be prevented successfully.
Raising Public Awareness
To build awareness on the subject matter, the use of social networks and similar digital tools will have to be considered. Specifically, the platforms in question will b utilized to build awareness and promote active education among women and girls. The specified step will allow the elimination of the damaging effects of misinformation that are currently present in the digital context. Similarly, the proposed solution will encourage the promotion of health education among the target population. As a result, women will be able to identify key threats to their health and require the necessary screening. Consequently, instances of cervical cancer will be identified and prevented successfully. Furthermore, essential interventions will be administered to the population at risk so that cervical cancer could be addressed accordingly at the earliest stages before it reaches the metastatic stage.
Even while not all cancers are unpleasant, pain can nonetheless be brought on by the disease or its treatment. Pain brought on by cancer can be adequately managed with medications and other methods. A sense of being out of breath might be brought on by cancer or cancer treatments (Allen et al. 2019).
Allen, E. M., Lee, H. Y., Pratt, R., Vang, H., Desai, J. R., Dube, A., & Lightfoot, E. (2019). Facilitators and barriers of cervical cancer screening and human papilloma virus vaccination among Somali refugee women in the United States: a qualitative analysis. Journal of Transcultural Nursing, 30(1), 55-63.
Chan, C. K., Aimagambetova, G., Ukybassova, T., Kongrtay, K., & Azizan, A. (2019). Human papillomavirus infection and cervical cancer: epidemiology, screening, and vaccination—review of current perspectives. Journal of oncology, 2019.
Fouly, H., & Hassen, S. (2020). Differences between the young and older married women regarding their knowledge and beliefs about cervical cancer running title: Women’s perspectives of cervical cancer . Egyptian Journal of Health Care, 11(4), 657-669. Web.
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2023, September 2). Community-Based Health Education on Cervical Cancer. https://ivypanda.com/essays/community-based-health-education-on-cervical-cancer/
"Community-Based Health Education on Cervical Cancer." IvyPanda , 2 Sept. 2023, ivypanda.com/essays/community-based-health-education-on-cervical-cancer/.
IvyPanda . (2023) 'Community-Based Health Education on Cervical Cancer'. 2 September.
IvyPanda . 2023. "Community-Based Health Education on Cervical Cancer." September 2, 2023. https://ivypanda.com/essays/community-based-health-education-on-cervical-cancer/.
1. IvyPanda . "Community-Based Health Education on Cervical Cancer." September 2, 2023. https://ivypanda.com/essays/community-based-health-education-on-cervical-cancer/.
Bibliography
IvyPanda . "Community-Based Health Education on Cervical Cancer." September 2, 2023. https://ivypanda.com/essays/community-based-health-education-on-cervical-cancer/.
- Capstone Project: HPV and Vaccination
- Cervical Cancer: Causes and Treatment
- Cervical Cancer and Risk Factors
- Human Papillomavirus Infection and Cervical Cancer
- The History of Cervical Cancer: Treatment and Care
- Cervical Cancer Prevention and Treatment Plan
- Cervical Cancer, Its Nature and Symptoms
- Human Papilloma Virus
- Vaccination Among HPV Virus
- Human Papillomavirus and Gardasil for Teenage Population
- Colorectal Cancer Screening and Its Effect on Disease Incidence
- The Burden of Cancer in the United States
- Statistical Analysis of Lung and Bronchus Cancer Data
- Pancoast Tumor: Neurological Symptoms and Comprehensive Treatment
- Garden Pesticide and Breast Cancer
- Share full article
Advertisement
Supported by
How to Avoid One of the Deadliest Forms of Skin Cancer
We asked experts what to know about melanoma symptoms, treatment and prevention.

By Ted Alcorn
When spring turns to summer and warm weather lures more people outside, skin cancer may be at most a distant concern. But experts said it’s important to take the risk seriously.
The ultraviolet rays in sunlight are a leading risk factor for skin cancer, which will affect one in five Americans over their lifetime. That includes melanoma, among the deadliest types. About 100,000 people are diagnosed with melanoma each year in the United States, and about 8,000 die from it annually, according to the American Cancer Society .
Fortunately, there are simple ways to reduce your risk, and to detect possible cases early while they are most curable. Therapies approved over the past 15 years have also transformed the treatment of melanoma, extending and improving the lives of patients even with late-stage cases.
Here’s what to know about melanoma, its treatments and how to protect yourself.
What is melanoma?
Melanoma is a cancer that typically starts in skin cells known as melanocytes that make the skin’s pigment. Compared with more common skin cancers that begin in squamous or basal cells, melanoma is more likely to spread to other parts of the body.
“It truly has a very aggressive behavior and biology behind it,” said Dr. Michael Davies, chairman of the melanoma medical oncology department at the University of Texas MD Anderson Cancer Center.
Most melanomas appear as flat or slightly elevated blotches of dark color on skin that has been frequently exposed to ultraviolet light, such as the scalp and face, arms, back and legs (though they can occur on areas that have never been exposed to the sun, too). In a smaller share of cases, the growth may appear as a dark- or red-colored bump and grow down into the skin, which can make it more difficult to detect.
A less common form, lentigo maligna melanoma, mostly afflicts older adults who have had significant sun exposure, and often appears as abnormally-shaped tan or brown spots on their heads or necks. An even rarer type, called acral lentiginous melanoma, occurs on the hands and feet (specifically the soles, palms, fingers, toes or nail beds) and accounts for more than half of melanoma cases in those who are not white. (The musician Bob Marley died from this type of melanoma, which was at first misidentified as a bruise.)
Melanoma can also occur in the eyes or mucosal membranes such as inside the nose or throat, but these cases are rare.
Who’s at risk? And can melanoma be prevented?
Melanoma is thought to be caused by a mix of genetic and environmental factors. One of the leading hazards is exposure to ultraviolet light, including from the sun and indoor tanning. A history of severe, blistering sunburns can raise your risk; as can living close to the Equator or at a high elevation, where the sun’s rays are more intense.
The best way to reduce your risk is to avoid unnecessary exposure to UV light. The sun’s rays are strongest between 10 a.m. and 4 p.m., so limit your time outside during those hours. Wear protective clothing and eyewear and regularly apply sunscreen of at least SPF 30 .
Dr. Shanthi Sivendran, a medical oncologist and senior vice president at the American Cancer Society, also warned against using tanning lamps and beds , which significantly increase melanoma risk. Twenty states and the District of Columbia have barred minors from using tanning beds, in part because of this concern, according to the Skin Cancer Foundation. But six states (Alaska, Colorado, Iowa, Montana, New Mexico and South Dakota) do not restrict them from doing so.
People with lighter skin are more vulnerable to damage from UV light. But Dr. Sivendran said that doesn’t mean those with darker skin shouldn’t also remain vigilant. “You can get melanoma regardless of what your skin color is,” she said.
It’s also important to know if melanoma runs in your family, which can heighten your risk. And people with compromised immune systems are also more likely to develop melanoma. While about half of cases occur in people aged 66 and over, younger people can also develop melanoma.
How can I detect melanoma?
Spotting melanoma early is vital, because nearly all cases that have not spread to other parts of the body are curable. However once the disease reaches the lymph nodes or more distant organs, five-year survival rates decrease significantly.
There are no standard guidelines for skin cancer screening, but clinicians can examine your skin for abnormalities during annual checkups. Dr. Kelly Nelson, a dermatologist at the MD Anderson Cancer Center, also recommended that patients conduct their own regular head-to-toe self exams .
To recognize changes in your skin, it’s helpful to be familiar with it, Dr. Nelson said. “People who are more aware of what the skin on their backs looks like are less likely to die of melanoma than people who have no clue at all.”
“It’s this fine line of balancing between having some degree of skin awareness, but also not being worried that every mole on your body is a ticking time bomb,” she added.
To distinguish melanomas from ordinary moles or irritations, dermatologists suggest checking for the “ABCDEs”: spots that have an asymmetrical shape, a notched or scalloped border, an unusual color pattern, a diameter larger than six millimeters, or a spot that has evolved over time.
In practice, however, Dr. Nelson said that patients often have trouble making these distinctions. She recommended looking out for “ugly ducklings,” meaning abnormalities that stand out for any reason .
How is melanoma treated?
For cancers that haven’t spread, a doctor will likely cut out the growth along with a margin of surrounding skin. They also may conduct a biopsy of nearby lymph nodes to assess the risk of the cancer spreading and help the doctor decide if further treatment is needed.
While melanoma is more likely to be deadly if it reaches distant parts of the body, major advances in treatment have improved the outlook, even for those who didn’t catch their cancer early.
These include treatments that harness the immune system to fight tumors, and targeted therapies that directly attack cancer cells.
There are more innovations on the way. In February, the Food and Drug Administration approved the first cancer treatment using tumor-infiltrating lymphocytes , known as TIL therapy, for use against melanomas that have not responded to other treatments. And scientists are also testing a vaccine tailored to the specific genetic makeup of a patient’s cancer in a late-stage clinical trial .
The Fight Against Cancer
Colon and rectal cancers are increasing among people younger than 50. Experts have a few ideas about why .
Should alcoholic beverages have cancer warning labels? Ireland will require them starting in 2026, and there are nascent efforts elsewhere .
Risk calculators can offer a more personalized picture of an individual patient’s breast cancer risk. But experts warn that the results need to be interpreted with the help of a doctor .
The human papillomavirus vaccine provides powerful protection against the leading cause of cervical cancer and against a strong risk factor for anal cancer. Here’s what to know about the shot .
A recent study adds to growing evidence that exercise is an important part of preventing prostate cancer , the second most common and second most fatal cancer in the United States for men.
No single food can prevent cancer on its own, but experts say that there are some that may help you build the best defense .
IMAGES
COMMENTS
Cervical cancer is the fourth most common cancer in women globally with around 660 000 new cases and around 350 000 deaths in 2022. The highest rates of cervical cancer incidence and mortality are in low- and middle-income countries. This reflects major inequities driven by lack of access to national HPV vaccination, cervical screening and ...
Introduction. Cervical cancer is the second common female malignant tumor globally which seriously threatens female's health. Persistent infection of high-risk human papillomavirus (HPV) has been clarified to be the necessary cause of cervical cancer (1,2).The clear etiology accelerated the establishment and implementation of comprehensive prevention and control system of cervical cancer.
2. Epidemiology of Cervical Cancer. Cervical cancer is a devastating malignancy of the cervix, with squamous cell carcinomas reported to be more prevalent than adenocarcinomas [10,11].The year 2020 recorded an estimated 604,000 new cases of cervical cancer and 324,000 deaths globally, with almost 90% of these cases occurring in low- and middle-income countries [2,12].
Globally, cervical cancer is the fourth most common female cancer after breast, colorectal, and lung cancer and accounts for 600 000 new cases and 340 000 deaths annually [ 1, 3, 4 ]. Importantly, approximately 83% of all new cervical cancer cases and 88% of all deaths occur in LMICs [ 3, 4 ]. Indeed, cervical cancer is the leading cause of ...
As it grows, cervical cancer might cause signs and symptoms, such as: Vaginal bleeding after intercourse, between periods or after menopause. Menstrual bleeding that is heavier and lasts longer than usual. Watery, bloody vaginal discharge that may be heavy and have a foul odor. Pelvic pain or pain during intercourse.
Cervical cancer ranks third among all new cancer cases and causes of cancer deaths in females. The paper provides an overview of cervical cancer prevention strategies employed in different regions, with incidence and mortality rates ranging from high to low. ... Over the past three years, at least 80 papers have been published on this topic.
About abnormal cells in the cervix that can become cancer. Cervical cancer begins when healthy cells on the surface of the cervix change or become infected with human papillomavirus (HPV) and grow out of control, forming a mass called a tumor. Long-term infection of HPV on the cervix can result in cancer, leading to a mass or tumor on the cervix.
Cervical cancer. Cervical cancer develops in a woman's cervix (the entrance to the uterus from the vagina). Almost all cervical cancer cases (99%) are linked to infection with high-risk human papillomaviruses (HPV), an extremely common virus transmitted through sexual contact. Although most infections with HPV resolve spontaneously and cause no ...
Globally, 570 000 cases of Cervical Cancer and 311000 deaths from the disease occurred in 2018. Cervical Cancer is the fourth most common cancer in women, ranking after breast cancer (2.1 million cases), colorectal cancer (0.8 million) and lung cancer (0.7 million). 1 It is the 2nd most leading cause of female cancer among women aged 15-44 years in India.
Cervical cancer continues to rank among the top gynecologic cancers worldwide. According to current data, it is ranked 14th among all cancers and is the 4th most common cancer among women worldwide.[1] Cervical cancer intervention focuses on primary and secondary prevention.[2] Primary prevention and screening are the best methods to decrease the burden of cervical cancer and mortality.
Cervical Cancer Case Study and Care Plan Cervical Cancer The following represents an outline for a plan of care, including information intended to educate the patient about what she can expect given her recent diagnosis of cervical cancer at the age of 45. The good news is that a cervical cancer diagnosis is no longer a death sentence. Cervical cancer in women is common and afflicts close to ...
INTRODUCTION Cervical cancer is a disease in which malignant (cancer) cells form in the tissues of the cervix or cervix uteri. Cervical cancer is the third most commonly diagnosed cancer and the fourth leading cause of cancer death in females worldwide with over 527,000 new cases 1,2 and perhaps the second most common cancer among women in the third world countries 3-5 It accounts for 9% of ...
Abstract. Each year, more than half a million women are diagnosed with cervical cancer and the disease results in over 300 000 deaths worldwide. High-risk subtypes of the human papilloma virus (HPV) are the cause of the disease in most cases. The disease is largely preventable. Approximately 90% of cervical cancers occur in low-income and ...
India. Abstract. Cervical cancer develops in a woman's cervix (the entrance to the uterus from the vagina). Almost all cervical cancer cases (99%) are linke d to infection with high-risk human ...
This page of the essay has 5,922 words. Download the full version above. Cervical cancer is the fourth most common malignancy affecting women worldwide, accounting for nearly 10% of all cancers (excluding non-melanoma skin cancers) and about 265,700 deaths annually (7.5% of all female cancer deaths) (1). This burden of disease exists in spite ...
Cervical cancer is a significant global health problem, with an estimated 604,127 new cases and 341,831 deaths worldwide in 2020, making it the fourth-most prevalent cancer among women [].Almost 90% of these deaths occur in low- and middle-income countries [].Africa has seen the highest incidence and mortality rate of cervical cancer, and countries in the region have bear a greater burden ...
The essay covers issues regarding cervical cancer. It sets off by introducing and presenting an overview of the disease and its severity among the female members of the society. According to the essay, cervical cancer is an outcome occasioned by the HPV virus. The HPV virus causes cervical cancer and is spread through sexual contact.
Yale Cancer Center (YCC) researchers at Yale School of Medicine (YSM) analyzed the genetic landscape of 66 tumors, the largest series of cervical NET ever reported in scientific literature. They used cutting-edge techniques (whole-exome and RNA-Seq analysis) to sequence all the genes from the tumors and identified the mutations that are crucial ...
The results of the meta-analysis show that the screening rates for all types of cancer were positively influenced by patient navigation. While studies analyzing cervical cancer were limited in number, the consistency of the results for the available sources and the outcomes for other types of cancer demonstrate the overall effectiveness of this approach (Vu, 2021).
1. Introduction. Cervical cancer is the fourth most common cancer in women worldwide, with an estimated incidence of 570,000 and 311,000 related deaths in 2018 [].Although the incidence of cervical cancer has declined in the United States, it remains the leading cause of cancer-related death in developing countries [].Thus, many recommendations on the screening, diagnosis, and treatment of ...
Causes of Cervical Cancer. Scientists have discovered that there is no single cause of cervical cancer. They believe that the interaction of several factors together caused cancer cells. The factors causing cervical cancer can be environmental, genetic, or at times caused by the genetic constitutional characteristics of a person.
Cervical Cancer Essay. Cervical cancer malignant cancer of the cervix uteris or cervical area. It may present with vaginal bleeding but symptoms may be absent until the cancer is in its advanced stages, which has made cervical cancer the focus of intense screening efforts using the Pap smear. About 2.2 percent of women carry one of the 2 virus ...
Cervical Cancer - Free Essay Examples and Topic Ideas . Cervical cancer is a type of cancer that develops in the cervix, which is the lower part of the uterus that connects to the vagina. It is usually caused by the human papillomavirus (HPV) and can be prevented through regular cervical cancer screenings and HPV vaccinations. Symptoms may ...
Introduction: Cervical cancer is the cancer of the lowest part of the uterus, which is known as cervix. Cervical cancer is very slow growing, but in some cases it can grow and spread quickly (Dolinsky & Hill-Kayser, 2009). There are many types of cervical cancer. The most common type is called squamous cell carcinoma (figure 1), which found in ...
The good news is that a cervical cancer diagnosis is no longer a death sentence. Cervical cancer in women is common and afflicts close to 530,000 women worldwide each year (Colombo et al., 2012). Importantly, human papillomavirus (HPV) infections are believed to be the most important causative agent and this virus is detected in 99% of all ...
In this study, we reviewed CT/MRI scans and studied the rates of radiation-related fractures in subjects treated for cervical cancer (CC, 63 subjects) by radical radiotherapy (RT) and in subjects treated for endometrial cancer (EC, 64 subjects) by radical surgery and RT. The differences between bone density measured in L1 on pretreatment CT, age and body mass index (BMI) were evaluated.
The ultraviolet rays in sunlight are a leading risk factor for skin cancer, which will affect one in five Americans over their lifetime. That includes melanoma, among the deadliest types. About ...