

Workshop on Disability in America: A New Look: Summary and Background Papers (2006)
Chapter: appendix b conceptual models of disability: past, present, and future--gale whiteneck, b conceptual models of disability: past, present, and future.
Gale Whiteneck *
I n the last quarter century, the conceptualization of disability has progressed dramatically. Two World Health Organization (WHO) international classification systems serve as bookends to this period. The WHO International Classification of Impairments, Disabilities, and Handicaps (ICIDH), 1 published in 1980, suggested conceptual distinctions among three levels of performance—impairment at the organ level, disability at the person level, and handicap at the societal level. However, ICIDH sparked controversy by labeling the societal level as “handicap” and by failing to incorporate environmental factors. Twenty-one years later, WHO published its revision of ICIDH as the International Classification of Functioning, Disability and Health (ICF), 2 which replaced the three dimensions with more appropriate labels (body structure and function at the organ level, activity at the person level, and participation at the societal level) and recognized the importance of environmental factors with a new categorization system.
Between these two events, several advances articulated the significant role of the environment in the lives of people with disabilities. The Americans with Disabilities Act 3 established full participation in society as the goal for all people with disabilities and ensured their right to reasonable accommodation to achieve it. The National Institute on Disability and
Rehabilitation Research provided the new paradigm of disability that focused attention on the imperative of environmental modifications to improve the lives of people with disabilities. 4 The Institute of Medicine’s (IOM’s) book Enabling America 5 promoted the importance of environmental factors for people with disabilities. Researchers focused their attention on the development of participation and environmental measures, including the Craig Handicap Assessment and Reporting Technique, 6 , 7 the Community Integration Questionnaire, 8 and the Craig Hospital Inventory of Environmental Factors. 9 , 10
Although the models theoretically incorporated the importance of environmental factors, little empirical evidence exists to support the theory. For example, spinal cord injury (SCI)-related research has linked impairment and disability to participation. Although the severity of the impairment had a strong relationship with the performance of activities of daily living, the research found no strong links between impairment or disability measures and participation. 11 , 12 A meta-analysis conducted by Dijkers 13 concluded that participation was more strongly related to quality of life than to either impairment or disability.
MODELS OF DISABILITY
Society’s and researchers’ conceptualizations of disability have evolved over time. As noted in Enabling America 5 and on the basis of public policy at the time, “In the 1950s, impairment of a given severity was viewed as sufficient to result in disability in all circumstances; in contrast, the absence of impairment of that severity was thought to be sufficient grounds to deny disability benefits” (p. 63) Although the practice of rehabilitation certainly existed before then, it was not until the 1960s and the 1970s that conceptual frameworks for modeling disability appeared. These conceptual frameworks allowed greater scientific inquiry into both disability and rehabilitation.
In 1972, WHO, recognizing a need for better methods to evaluate health care, sought to expand the medical model of illness that provided the basis for its International Classification of Disease (ICD). 14 WHO recognized that ICD 14 suited the study of the outcomes of acute diseases and injuries that can be prevented or cured but that the medical model did a woefully inefficient job of detecting the consequences of nonacute diseases, particularly chronic and progressive or irreversible disorders. In 1980, WHO published ICIDH 1 as “a manual of classification relating to the consequences of disease.” It extended the disease-related sequence of etiology, pathology, and manifestation with the illness-related sequence of disease, impairment, disability, and handicap. Although the original ICIDH model acknowledges a role of the environment by stating that “handicaps thus reflect interaction with and adaptation to the individual’s
surroundings,” it has been criticized for its lack of an explicit recognition of the environmental role in its model.
Nagi 15 also recognized the process by which a pathology (e.g., arthritis) may lead to an impairment (e.g., limited joint range of motion), which may then result in a functional limitation (e.g., an inability to type), which ultimately may result in disability (e.g., an inability to work as a secretary). Possibly because of his attention to employment rather than health care services, Nagi noted that correlations among impairments, functional limitations, and social roles, such as employment, were poor. Unlike ICIDH, Nagi’s model explicitly recognized that the environment could be studied separately from the individual and initiated research into environmental factors in the family, the community, and society that affect disability as an outcome. Fougeyrollas 19 further clarified the influence of environmental factors on social participation in a manner consistent with the Nagi approach.
Verbrugge and Jette 16 proposed an expanded model of the disablement process to account for behaviors and attributes that increase the risks of or that provide buffers to functional limitations and disability, elements not specified in Nagi’s medical model. Relevant factors include both intra-individual characteristics (e.g., behavioral change and locus of control) and extraindividual characteristics (e.g., medical care, environmental barriers or adaptations, and instrumental support) that may operate at various points along the disablement trajectory.
IOM, in Disability in America , 17 derived its conceptual model of disability directly from Nagi and, in fact, defined disability “by the attributes and interactions of the individual and the environment” (p. 82). In the IOM model, risk factors exist not only within the individual but also in the physical and social environments, all of which theoretically affect the disability process. In the more recent IOM report, Enabling America , 5 the conceptual model was modified to emphasize that “the environment plays a critical role in determining whether each stage of disablement occurs and if transitions between the stages occur” (p. 64). The National Center for Medical Rehabilitation Research (NCMRR), in its research plan for the National Institutes of Health, 18 also emphasized the environment by use of a category of function called “societal limitations,” which it defined as “restrictions attributable to social policy or barriers (structural or attitudinal) which limit fulfillment of roles or deny access to services and opportunities associated with full participation in society” (p. 25).
In addition to environmental factors, some researchers have argued that personal factors such as age, gender, and race also deserve separate consideration in disability theory. Personal factors may appear to be separate features of the individual distinct from a particular health condition or health state, yet they may influence the disability process. Such factors may also include variables such as habits, lifestyles, experiences, coping styles,
and other psychological assets that may play a confounding role in the structural modeling of disability. 19
WHO’s ICF provides the most recent and, arguably, most comprehensive model of disability. 2 It revises the earlier ICIDH 1 by using less pejorative language (e.g., “participation” replaces “handicap” as a functional domain), explicitly incorporating environmental and personal factors as “contextual factors” that affect disability outcomes, and recognizing multiple levels and directions of potential causal relationships. Table B.1 summarizes key models of disability and illustrates the confusion attributable to the inconsistent terminology used to label conceptual domains.
ICF DOMAINS OF DISABILITY
WHO designed ICF 2 to achieve a better scientific understanding of health and health outcomes. ICF provides a common language of health to enable sharing of data among countries and health care providers. ICF describes broad health-related domains that can be transformed into a meaningful and consistent coding system. The ICF Model of Disability 2 is depicted in Figure B.1 .
ICF has two parts: Part 1 covers functioning and disability, and Part 2 deals with contextual factors. Components of functioning and disability include body function and structure, activities, and participation. Components of contextual factors include environmental factors and personal factors. The model conceives these components as separate but related constructs with dynamic interactions between health conditions, like disease, disorders, and injuries, and contextual factors, such as personal and environmental factors.
Describing the model component body functions and structure, ICF refers to the “body” as the human organism. It includes not only physical aspects of the human body but mental functions as well. Body functions encompass the physiological and psychological functions of body systems. Body structures include the anatomical parts of the body, including the limbs and organs. ICF defines impairment as a problem in the body function or structure that results in a significant deviation or loss. Impairment does not always indicate the presence of disease and has a broader and more inclusive scope than disease. Impairments may cause other impairments; for example, impaired brain function may cause impaired cognitive function.
The ICF graphic model ( Figure B.1 ) differentiates between the second and the third levels, activities and participation. 2 Activities refer to “the execution of a task or action by an individual,” and participation refers to “involvement in a life situation.” Examples of activities include listening, walking, and eating. Participation items describe roles that people perform,
TABLE B.1 Concepts and Terminology Used by Models of Disability
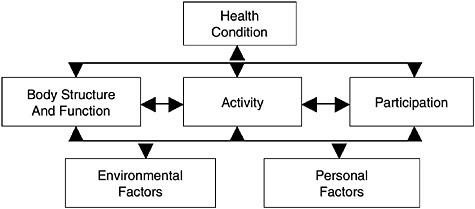
FIGURE B.1 ICF model of disability. 2
such as forming relationships with others, caring for a household, or seeking and maintaining employment.
Although ICF depicts activities and participation separately in the graphic model, it uses one coding structure for both and covers the major areas of activity that one encounters throughout a life span. The list of domains includes learning and the application of knowledge, general tasks and demands; communication; mobility; self-care; domestic life; interpersonal interactions and relationships; major life areas; and community, social, and civic life. ICF defines difficulties as activity limitations or participation restrictions and measures them by comparing the performance of an individual with a health condition (a disease, injury, or disorder) with that of an individual without the condition. The difference between what one actually sees and what one expects to see provides a measure of the limitation.
One of two contextual components of ICF, environmental factors, includes the physical, social, and attitudinal environments, or the external factors of an individual’s life. These factors can have either a negative influence (“barrier”) or a positive influence (“facilitator”) on a person’s performance in society, on an individual’s ability to carry out tasks, or on an individual’s body function and structure. ICF organizes environmental factors into two levels: individual and societal. Individual environmental factors include the immediate environment of the individual, such as home and work: the physical or material features of the environment, as well as the individual’s interaction with family, peers, acquaintances, and strangers. Societal factors include formal and informal services and systems in the community that affect a person’s life. Societal factors encompass organizations and services related to work, community activities, government agencies, communication services, and transportation services.
Finally, ICF 2 identifies personal factors as “the particular background of an individual’s life and living, and comprises features of the individual that are not part of health condition or health states” (p. 17). For example, these factors include gender, minority status, age, lifestyle, habits, upbringing, coping styles, education, profession, personality characteristics, marital status, and overall behavioral patterns. All of these factors may play a role in disability at any level, and although ICF does not classify these factors because of the large social and cultural variances that exist within them, it acknowledges their potential importance.
Although much progress has been made in refining disability models, categories of function, and the role of the environment, 1 , 20 , 21 only limited quantitative studies 22 , 23 , 24 have attempted to validate the models.
SUMMARY AND CRITIQUE OF ICF
This author’s assessments of ICF compared with past models and the models of disability that are needed in the future can be summarized in the following title used in a recent presentation: “The ICF, one step forward, one step back, and a few steps yet to go for a complete model.” 25 The one step forward was the inclusion of environmental factors; the one step back was the blurring of activities and participation; and the needed steps include the differentiation of activities and participation, the addition of quality of life to the model, elaboration of the impact of environmental factors, the development of personal factors, refinement of the graphic depiction of the model, definition of research strategies to better measure the domains of disability, and validation of the model.
Background on the Revision of ICF
ICF lists hundreds of people from scores of countries who were involved in the decade-long revision process. The author’s comments here reflect a view of that process as gleaned from attendance at dozens of North American and international meetings. Although several cosmetic changes were made to ICIDH in the revision to ICF, substantive changes were also made. The cosmetic changes that occurred in the revision to ICF were the relabeling of the domains. That was necessary from the U.S. standpoint because the term “handicap” was completely unacceptable to the disability advocacy community because of its pejorative nature. ICF made an effort to use labels that were more neutral in tone, so “impairment” became “body structure and function,” disability became “activity,” and “handicap” became “participation.” The underlying cause of all of these outcomes was relabeled “health condition,” and there was recognition that this process was not a simple linear progression but included many interactions, so
numerous arrows were added to the model. Finally, the label of the model was changed to the model of functioning and disability. That brought the model to a point where the same basic underlying concepts had simply been relabeled, but now a set of labels that would be acceptable in the United States and that were less negative toward people with disabilities was being used.
The Step Forward
The addition of environmental factors was the major step forward in this process, and among the U.S. delegation this was the highest priority. In fact, without that addition, the model would have remained unacceptable to disability advocacy groups and therefore would not have been used. The addition of environmental factors was the major part of adding broader contextual factors that included both environmental and personal factors. It took a few years for environmental factors to be incorporated into the draft model, and they seemed to slip out and periodically needed championing to keep them in. Eventually, they were maintained, and in the author’s view, that was probably the major step forward in the conceptualization of disability outcomes.
The Step Backward
The loss of a clear distinction between activity and participation was the step backward. In the development of the category schemes and in the listing of the elements of the domains of activity and participation, there were disagreements. One school of thought was that everything is an activity and the issue is just one of the complexity of the activity. Therefore, for that group, the desire was to have a very long list of activities. From the U.S. perspective and the perspective of the delegations from other English-speaking countries, there was a desire to maintain the concept of participation in terms of performance as a member of society—working, going to school, parenting, and socializing—as a separate and distinct dimension. This was controversial. In the preliminary draft that was tested, a distinction between activity and participation was made; and a list of activities, as well as a list of participation, was made. Although there were disagreements about whether something was an activity or participation, a consensus on how to resolve these controversies was starting to develop among the delegations from the English-speaking countries. At the last minute, however, WHO decided to say that activity and participation both have the same elements. That resulted in one list of elements for the combined activity and participation domain—a decision that blurs the distinction between activity and participation.
The problem was further complicated by the last-minute introduction of two qualifiers to these dimensions—capacity and performance—with the implications that capacity was related to activity and that performance was related to participation. Furthermore, the suggestion that capacity should be measured in a uniform standard environment whereas participation should be measured in the real world also added confusion to the conceptual model.
SEVEN STEPS TO IMPROVE THE MODEL
It is the view of the author that seven steps are warranted to improve the present ICF Model of Disability. These steps represent conceptual clarifications and enhancements as well as research strategies that can be used to implement and validate the model. Both conceptual and empirical advances are needed to move the disability field forward. These advances are envisioned as iterative processes, in which the conceptual model guides research and empirical evidence informs theory, which culminate in a revised and validated Model of Disability (ICF-2). Continuing empirical work must proceed, without waiting for a perfect model, to inform theoretical perspectives. On the other hand, improved conceptualizations will guide the disability field. In the author’s view, the primary role of ICF and its revisions are to guide and evaluate research, policy, and practice rather than to serve as a classification scheme. Although implementation of the proposed revisions will be a challenge, they will be worth the effort and will lead to a better theoretical understanding of disability, which, in turn, can improve the lives of people with disabilities.
Step 1: Distinguishing Activity and Participation in the Next Model Revision
The blurring of activity and participation was a step backward that must be repaired. In the next revision of ICF, distinctions between activity and participation need to be clarified as the first step in improving the present model.
Several themes differentiate these two important concepts. First, and most importantly, activity is at the individual person level, whereas participation is at the societal level. Activities are more likely to be performed alone, whereas participation elements would more likely be performed with others. In some sense, activity is a simpler concept, whereas participation is a more complex process. Activity is related more closely to the extent of impairment, whereas participation is related more closely to perceived quality of life. Meta-analysis 13 demonstrates that the severity of the impairment is highly correlated with activities of daily living but is not strongly related
to quality of life, whereas participation is more closely related to quality of life. Activity may be thought of as less environmentally dependent, whereas participation is more environmentally dependent. Although, conceptually, environmental factors play a role in both levels, it does seem clear that participation is the area that is the most influenced by the environment. Activity is embraced by the medical model of disability, whereas participation emerges from a social model of disability. The measurement of activity is a focus of rehabilitation, whereas the measurement of participation reflects the outcomes most important to individuals with disabilities, their family members, and society. Activity is more typically assessed in a rehabilitation setting, whereas participation should be assessed in the community setting. Activity is more often assessed by a clinician or professional, whereas participation is more often a self-report of the individual with a disability. Finally, in the current state of the science, all activity limitations cannot yet be eliminated, but theoretically, most participation restrictions can be eliminated. Although all disabilities cannot be cured, society is in a position, at least theoretically, to return people to active, productive lives that are well integrated into family and community life. Society is better prepared to maximize participation than to maximize activity.
Nagi made a strong conceptual basis for differentiating activities and participation in Appendix A of Disability in America , 2 in which he attempted to clarify the distinction between performance at the level of the person (which he called “functional limitations”) and performance at the societal level (which he called “disability”). For Nagi, role performance was the defining concept at the societal level. He, like Parsons, 26 viewed “role performance” as an organized system of participation by an individual in a social system, whereas tasks are more specialized than roles and can be viewed as subsystems of roles. Nagi argued that activities of daily living are task behaviors that are parts of (but different from) role expectations inherent in a person’s family, vocational, and social lives. Furthermore, Nagi suggested that tasks or activities were attributes or properties of individuals in isolation, whereas roles and participation were relational concepts requiring consideration of environmental factors in which the roles were performed. This early conceptual focus on roles as the defining characteristic of performance at the societal level may offer an effective way to differentiate activities and participation in ICF-2.
Step 2: Quality of Life, a Key Missing Component of ICF
ICF offers a comprehensive model of objective disability outcomes and provides rehabilitationists and researchers with a system for categorizing disability. However, it does not address the subjective perceptions and preferences of people with disabilities. It is for this reason that disability
researchers have criticized ICF for lacking a subjective dimension and recommended augmentation of ICF with an additional dimension—quality of life 25 —as the second step in the revision of ICF.
Although WHO does not include the concept of quality of life in the ICF Model of Disability, it has recognized both the importance of the quality-of-life concept and its relationship to disability outcomes. WHO defined quality of life as “the perception of individuals of their position in life, in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns.” 27 According to WHO, the determinants of quality of life include the consequences of disability, particularly handicap or participation. 1 On the basis of WHO documents, Barbotte and colleagues described quality of life as a wide-ranging concept “affected by people’s social relationships, physical health, psychological state and level of independence, and by their relationship to salient features of their environment” 28 (p. 1048).
Quality of life, defined as a self-appraisal of subjective well-being or life satisfaction made by the person with a disability, might be acknowledged by the ICF WHO Model of Disability in one of three ways: (1) it could be added as a separate domain to the right of participation, indicating that the extent of quality of life is the ultimate outcome of the disability process; (2) it could be added as a qualifier to each of the present domains of ICF, indicating that satisfaction with participation, activities, and even body structures and functions is an important aspect of disability; or (3) it could be excluded from the model itself but acknowledged as a key life outcome influenced by the disability process. This author favors the first approach. The exclusion of quality of life from the model but acknowledgment of its importance fails to require that the subjective assessment of the individual with a disability be included in any comprehensive assessment of disability. The incorporation of a subjective satisfaction qualifier as part of each current domain adds conceptual confusion to each of the domains and fails to focus attention on a unique outcome of critical importance. Only the actual addition of a new quality-of-life domain acknowledges the validity of the subjective perceptions of people with disabilities and that those perceptions are distinct outcomes of the disability process.
Quality of life could be measured simply by using a standardized assessment of global life satisfaction 29 or an instrument that assesses satisfaction with domains of life; 30 but it should not be a composite measure of Health-Related Quality of Life (HRQOL), including impairment, activity limitation, participation restriction, and quality-of-life indicators, as is often the case with HRQOL measures. 31 The author suggests that the inclusion of a new quality-of-life domain is more important than the addition of a quality-of-life taxonomy with a coding system. Furthermore, the potential difficulty of adding a new domain and the complexity that it brings will be
outweighed by the conceptual importance of the subjective assessment by the person with a disability. Quality of life was first recognized as an important domain by Enabling America , 5 and its addition to ICF is a critical revision.
Step 3: Elaborating the Complexity of Environmental Factors
The third step needed in the revision of ICF is elaboration of environmental factors. It was a tremendous step forward to acknowledge the role of environmental factors. The environmental factors research that has been done has given some insight into the relationship between environmental factors and participation. Conceptually, models have always suggested that the more barriers that people encounter, the lower their participation is and that barriers actually prevent people from participating in society. On the other hand, the theories suggest that the more facilitating the environment is, the more likely it is that people with disabilities will fully participate in society. In initial environmental research, most correlations between environmental barriers and participation were negative, as expected. However, it was a surprise to find a few positive correlations between some environmental factors and participation, indicating a more complex relationship. The data seemed to suggest that when people encounter barriers, their participation is less; but they also suggest that for those people who persevered and got out and involved in the community and fully participated, they also witnessed and perceived more environmental barriers. It is not a simple one-way relationship.
Only two disability studies have systematically examined environmental barriers and their relationship to other ICF concepts and quality of life: one in traumatic brain injury (TBI) 32 and one in SCI. 24 The TBI study surveyed 73 participants from one TBI model system program at their first anniversary of injury, with respondents reporting a greater impact from environmental barriers also reporting lower levels of participation and life satisfaction. 32
The SCI study surveyed 2,726 participants from the 16 federally designated SCI model systems as they crossed their 1st, 5th, 10th, 15th, 20th, or 25th anniversary of injury. Environmental barriers accounted for only 4 percent of the variation in participation, but they accounted for 10 percent of the variation in quality of life. The SCI study supported the inclusion of environmental factors in models of disability, like ICF, but concluded that environmental factors had a stronger relationship to quality of life than they did to societal participation. 24 This last finding of the SCI study raises the pivotal question: do environmental factors directly influence participation, which in turn influences quality of life, or do environmental factors more directly influence quality of life? Environmental barriers may reduce
participation, or the struggle to overcome barriers and fully participate may reduce quality of life. There is much to learn about the actual role of environmental factors in the disability process, and researchers need to develop some theory underlying the concept that helps explain under what conditions barriers actually mean that participation does not occur and under what conditions people move beyond those barriers and participate. Considerable theory building will be required to accomplish this third step in revising ICF.
Step 4: An Understanding and Taxonomy of Personal Factors
The fourth step needed to improve ICF is the development of personal factors. However, this step is controversial. The current conceptual model acknowledges that contextual factors, including both environmental and personal factors, play a major role in disability outcomes. Environmental factors are considered everything external to the individual—physical, attitudinal, and policy factors. Personal factors should be thought of as all of the factors that are internal to the individual but unrelated to the disability itself, including the preexisting conditions, demographic factors, and personal characteristics that existed before an impairment occurred or that are not directly related to the disabling process. Looking for demographic differences in disability outcomes is an area in which investigators are comfortable, but efforts to venture into the arena of personal factors beyond demographics have not been made. Psychological factors and personality factors are seldom examined, possibly for reasons of political correctness. The concern of advocacy groups is that if it begins to be suggested that motivation or compliance with treatment is an important factor in producing disability outcomes, then the field is precariously on the verge of once again suggesting that the problem lies with the individual instead of the environment. Advocacy groups would then once again challenge the medical model because it failed to consider environmental factors. Therefore, it is critical that people with disabilities and advocacy groups be fully involved in any development of a personal factors taxonomy. Furthermore, careful consideration will be needed when something that might seem to be a personal factor might better be viewed as psychological structure or function. However, eventually, to have a complete model that is able to predict a major portion of the variances in outcomes, personal factors will likely need to be included. Therefore, the development of a personal factors taxonomy with a better theoretical understanding of the significance of personal factors needs to be one of the steps in the ICF revision process.
Step 5: Refining a Graphic Representation of the Model
Neither the complex diagram of multiheaded arrows and boxes of ICF nor the “man on the mat” diagrams in Enabling America provide a clear depiction of the interaction of health conditions with contextual factors that produce disability outcomes. If a more compelling graphic depiction that clarified the nature of conceptual relationships in an intuitive manner could be developed, the more widespread adoption of the revised model would be more likely. Refining the graphic is therefore listed as the fifth step in revising the ICF.
Step 6: Developing Improved Measures of the Domains of Disability
The final two steps advocated for advancing the conceptual understanding of disability have more to do with the application of the model than its revision. Both current and future models of disability require extensive testing. The reliability and practicality of the taxonomy must be evaluated, but more importantly, the implied relationships among the concepts must be assessed. A prerequisite of that task is the availability of psycho-metrically sound measures of the ICF concepts. Although many measures of impairment and activities of daily living have been developed, the measurement of participation is a relatively new field and the measurement of environmental factors is in its infancy. Considerable psychometric evaluation of existing and newly developed instruments is needed to reach a consensus on standardized methods of quantifying each of the domains of the disability. Major surveys need to incorporate reliable and valid measures specifically designed to assess the conceptual domains of ICF rather than simply trying to retrofit existing survey questions to the ICF taxonomy by developing “crosswalks” to ICF codes.
Step 7: Validate the Model
Once valid and reliable tools are developed, they can be applied in multivariate analyses to determine the strength of relationships among ICF concepts. Replication of such work with multiple populations with different impairments will be needed. The development of a research strategy to tackle this problem would be a significant step and contribution to the field, but full validation of the model also requires the use of the model to guide interventions to improve the lives of people with disabilities. Therefore, the final step includes the design, implementation, and rigorous evaluation of interventions based on the conceptual model. The ultimate test of a model is whether it facilitates effective interventions. The revised conceptual model,
in combination with the empirical tests of the model, should provide the information necessary to direct effective interventions.
CONCLUSIONS
As IOM begins the process of reconsidering its seminal works Disability in America and Enabling America , published nearly 15 and 10 years ago, respectively, clear advances have occurred in the conceptualization of disability, but more work is needed in clarifying concepts. WHO’s ICF has incorporated a major concept advocated by Enabling America —environmental factors—and ICF, as the currently accepted international model, should be the starting point for advocating future conceptual revisions. Seven steps have been outlined to improve the ICF conceptualization, including the differentiation of activities and participation, the addition of quality of life to the model, elaboration of the impact of environmental factors, the development of personal factors, refinement of the graphic depiction of the model, definition of research strategies to better measure the domains of the model, and validation of the model by testing the interrelationships among its concepts and deriving interventions to improve the lives of people with disabilities.
1. World Health Organization. International Classification of Impairments, Disabilities and Handicaps: a Manual of Classification Relating to the Consequences of Disease . Geneva, Switzerland: World Health Organization; 1980.
2. World Health Organization. International Classification of Functioning, Disability, and Health . Geneva, Switzerland: World Health Organization; 2001.
3. The Americans with Disabilities Act. P.L. 101-336. 1990.
4. National Institute on Disability and Rehabilitation Research. National Institute on Disability and Rehabilitation Research (NIDRR) Long Range Plan for Fiscal Years 1999-2003. Web Page. Available at http://www.ncddr.org/new/announcements/nidrr_lrp/index.html . Last accessed October 18, 2005.
5. Institute of Medicine. Enabling America: Assessing the Role of Rehabilitation Science and Engineering . Washington, DC: National Academy Press; 1997.
6. Whiteneck GG, Charlifue SW, Gerhart KA, Overholser JD, Richardson GN. Quantifying handicap: a new measure of long-term rehabilitation outcomes. Archives of Physical Medicine and Rehabilitation 1992; 73:519–526.
7. Whiteneck G, Brooks C, Charlifue S, et al. Guide for Use of CHART: Craig Hospital Assessment and Reporting Technique . Englewood, CO: Craig Hospital; 1992.
8. Willer B, Rosenthal M, Kreutzer J, Gordan W, Rempel R. Assessment of community integration following rehabilitation for traumatic brain injury. Journal of Head Trauma and Rehabilitation 1993; 8:75–87.
9. Craig Hospital Research Department; Craig Hospital Inventory of Environmental Factors (CHIEF) Manual , Version 3.0. Englewood, CO: Craig Hospital; 2001.
10. Whiteneck G, Harrison-Felix C, Mellick D, Brooks C, Charlifue S, Gerhart K. Quantifying environmental factors: a measure of physical, attitudinal, service, productivity and policy barriers. Archives of Physical Medicine and Rehabilitation 2004; 85:1324–1335.
11. Whiteneck G. Outcome analysis in spinal cord injury rehabilitation. In: Rehabilitation Outcomes: Analysis and Measurement . Fuhrer MJ, ed. Baltimore, MD: Paul H. Brookes Publishing Co.; 1987:221–231.
12. Whiteneck G. Outcome evaluation and spinal cord injury. NeuroRehabilitation 1992; 2:31–41.
13. Dijkers M. Quality of life after spinal cord injury: a meta analysis of the effects of disablement components. Spinal Cord 1997; 35:829–840.
14. World Health Organization. International Classification of Disease , 9th Revision. Clinical Modifications . Ann Arbor, MI: Commission of Professional and Hospital Activities; 1986.
15. Nagi SZ. An epidemiology of disability among adults in the United States. The Milbank Memorial Fund Quarterly 1976; 54:439–467.
16. Verbrugge LM, Jette AM. The disablement process. Social Science & Medicine 1994; 38:1–14.
17. Pope A, Tarlov A. Disability in America: Toward a National Agenda for Prevention . Washington, DC: National Academy Press; 1991.
18. National Institutes of Health. Research Plan for the National Center for Medical Rehabilitation Research . NIH Publication 93-3509. Washington, DC: U.S. Department of Health and Human Services; 1993.
19. Fougeyrollas P. Documenting environmental factors for preventing the handicap creation process: Quebec contributions relating to ICIDH and social participation of people with functional differences. Disability and Rehabilitation 1995; 17:145–153.
20. Fougeyrollas P. Explanatory models of the consequences of disease and trauma: the handicap creation process . ICIDH, International Network 1993:6.
21. Whiteneck G, Fougeyrolles P, Gerhart G. Elaborating the model disablement. In: Assessing Medical Rehabilitation Practices: the Promise of Outcomes Research . Fuher M ed. Baltimore, MD: Paul H. Brookes Publishing Co.; 1997:91–102.
22. Heinemann A, Whiteneck G. Relationships among impairment, disability, and life satisfaction in persons with traumatic brain injury. Journal of Head Trauma Rehabilitation 1995; 10:54–63.
23. Hall MK, Hamilton BB, Gordon WA, Zasler N.D. Characteristics and comparisons of functional assessment indices: Disability Rating Scale, Functional Independence Measure, and Functional Assessment Measure. Journal of Head Trauma Rehabilitation 1993; 8:60–74.
24. Whiteneck G, Mead M, Dijkers M, Tate D, Bushnik T, Forchheimer M. Environmental factors and their role in participation and life satisfaction after spinal cord injury. Archives of Physical Medicine and Rehabilitation 2004; 85(11):1793–1803.
25. Whiteneck G. The ICF: one step forward, one step back, and a few steps to go to a complete model. Presentation to conference on State of the Science: Outcome Research in Post-Acute Care . April 24-25, 2003, Washington, DC. Organized by Boston University. Web Page. Available at http://www.bu.edu/cre/webcast/testwhiteneck.doc . Last accessed October 18, 2005.
26. Parsons, T. Definitions of health and illness in the light of American values and social structure. In: Patients, Physicians and Illness . Jaco EG, ed. Glencoe, IL: Free Press; 1958.
27. World Health Organization. Study protocol for the World Health Organization project to develop a quality of life assessment instrument: WHOQOL. Quality of Life Research 1993; 2:153–159.
28. Barbotte E, Guillemin F, Chau N. Prevalence of impairments, disabilities, handicaps, and quality of life in general population: a review of recent literature. Bulletin of the World Health Organization 2001; 79(11):1047–1055.
29. Diener E, Emmons R, Larsen J, Griffin S. The Satisfaction with Life Scale. Journal of Personality Assessment 1985; 49(1):71–75.
30. Flanagan J. A research approach to improving our quality of life. American Psychologist 1978; 33:138–147.
31. Ware J, Sherbourne C. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Medical Care 1992; 30:473–483.
32. Whiteneck G, Gerhart K, Cusick C. Identifying environmental factors that influence the outcomes of people with traumatic brain injury. Journal of Head Trauma Rehabilitation 2004; 19(3):191–204.
Beginning in late 2004, the IOM began a project to take a new look at disability in America. It will review developments and progress since the publication of the 1991 and 1997 Institute reports. For technical contracting reasons, the new project was split into two phases. During the limited first phase, a committee appointed by IOM planned and convened a 1-day workshop to examine a subset of topics as background for the second phase of project. As was agreed upon with the sponsor of the workshop, the Centers for Disease Control and Prevention (CDC), the topics were:
- methodological and policy issues related to the conceptualization, definition, measurement, and monitoring of disability and health over time;
- trends in the amount, types, and causes of disability;
- disability across the age spectrum and in the context of normal aging; and
- secondary health conditions.
The phase-one workshop was held in Washington, D.C. on August 1, 2005. Its participants included researchers, clinicians, social service professionals, policy experts, and consumer representatives and advocates. The meeting agenda and list of participants are included in Appendix A. Workshop on Disability in America: A New Look- Summary and Background Papers summarizes the workshop presentations and discussions. The background papers prepared for the workshop are included in Appendixes B through O. Some papers were submitted and circulated in advance of the meeting, whereas others were first presented at the meeting. The analyses, definitions, and views presented in the papers are those of the paper authors and are not necessarily those of the IOM committee. Likewise, the discussion summary is limited to the views of the workshop participants.
READ FREE ONLINE
Welcome to OpenBook!
You're looking at OpenBook, NAP.edu's online reading room since 1999. Based on feedback from you, our users, we've made some improvements that make it easier than ever to read thousands of publications on our website.
Do you want to take a quick tour of the OpenBook's features?
Show this book's table of contents , where you can jump to any chapter by name.
...or use these buttons to go back to the previous chapter or skip to the next one.
Jump up to the previous page or down to the next one. Also, you can type in a page number and press Enter to go directly to that page in the book.
Switch between the Original Pages , where you can read the report as it appeared in print, and Text Pages for the web version, where you can highlight and search the text.
To search the entire text of this book, type in your search term here and press Enter .
Share a link to this book page on your preferred social network or via email.
View our suggested citation for this chapter.
Ready to take your reading offline? Click here to buy this book in print or download it as a free PDF, if available.
Get Email Updates
Do you enjoy reading reports from the Academies online for free ? Sign up for email notifications and we'll let you know about new publications in your areas of interest when they're released.

- Table of Contents
- Random Entry
- Chronological
- Editorial Information
- About the SEP
- Editorial Board
- How to Cite the SEP
- Special Characters
- Advanced Tools
- Support the SEP
- PDFs for SEP Friends
- Make a Donation
- SEPIA for Libraries
- Entry Contents
Bibliography
Academic tools.
- Friends PDF Preview
- Author and Citation Info
- Back to Top
Disability: Definitions and Models
Philosophers have always lived among, and often as, people who could not see, walk, or hear; who had limited mobility, comprehension or longevity, or chronic illnesses of various sorts. And philosophers have lived in societies that respond to these and other bodily differences in a wide variety of ways. And yet philosophical interest in these conditions and the social response to them was piecemeal and occasional until the past hundred or so years. Some of these conditions were cited in litanies of life’s hardships or evils; some were the vehicle for inquiries into the relationship between human faculties and human knowledge (see entry on Molyneux’s problem ). But the treatment of disability as a subject of philosophical interest in its own right is relatively new.
The lack of attention to “disability” or the related concept of “impairment” may have a simple explanation: there were no such concepts to attend to until nineteenth century scientific thinking put variations in human function and form into categories of abnormality and deviance. Once such categories were established, it became possible to talk, and generalize, about (first) “the disabled”, and (then) “their impairments”, and philosophers have done so for various purposes [Hacking, 1990; L. Davis, 2002: Ch. 4]). The resurgent political philosophy of the second half of the last century, preoccupied with eliminating or reducing unearned disadvantages, tended to treat disability as a primary source of those disadvantages, to be addressed with medical correction or government compensation (Cohen 1993; Sen 1993). Somewhat later, social philosophers began to see disability as a source both of discrimination and oppression, and of group identity, akin to race or gender in these respects. And biomedical and other practical applied’ ethicists have been concerned to help policy-makers construct and interpret new legal and regulatory frameworks making central reference to “disability” and related concepts.
For these reasons and others, philosophers have had much to say, initially in passing and now at length, about what disability is and what “disability” means. This entry will discuss both issues—first, detailing philosophical engagement with longstanding debates over the correct “model” or general framework for understanding disability as a phenomenon; second, asking how philosophers have come to understand the meaning of concepts denoted by words like “disability” and “impairment”, as those have been used in various empirical and normative discourses concerning people with disabilities.
1.1 Medical and Social Models
1.2 an affirmative model, 1.3 models, decisions, and policies, 2.1 philosophical discussion of official definitions of disability, 2.2.1 normal-function views, 2.2.2 the welfarist view, 2.2.3 social constructionisms, 2.2.4 inability views, 2.2.5 skepticism about defining disabilities, other internet resources, related entries, 1. models of disability.
Many different characteristics have been considered disabilities. Paraplegia, deafness, blindness, diabetes, autism, epilepsy, depression, and HIV have all been classified as “disabilities”. The term covers such diverse conditions as the congenital absence or adventitious loss of a limb or a sensory function; progressive neurological conditions like multiple sclerosis; chronic diseases like arteriosclerosis; the inability or limited ability to perform such cognitive functions as remembering faces or calculating sums; and psychiatric disorders like schizophrenia and bipolar disorder.
Disabilities like these have been objects of study in sociology, medicine, and policy debates for much longer than they have been subjects of sustained interest in philosophy. These discourses do not tend to define “disability” by way of the sort of rigorous necessary and sufficient conditions philosophers often prefer. But they have been centrally concerned with broadly definitional issues, often discussed under the heading of “models” of disability—that is, general theoretical perspectives concerned to say what in the world social scientists are investigating when they investigate disability. These models generally pick out, both (1) a set of phenomenon as what needs explaining, when we explain disability, phenomenon typically but not necessarily characterized as disadvantages ; and (2) an explanation of these phenomenon—again, typically, but not solely, an explanation of why disabled people experience the disadvantages they do.
In their extreme forms, the medical and social models serve to chart the space of possible relationships between bodily difference and functional limitation more than to reflect the actual views of individuals or institutions. (A variety of more formal models, described in Altman 2001, graphically represent the causal complexity of disability.)
The medical model explains disability disadvantage in terms of pathological states of the body and mind themselves. It regards the limitations faced by people with disabilities as resulting primarily from their bodily differences. The medical model is rarely defended explicitly, but aspects of it are often adopted unreflectively, when health care professionals, bioethicists, and philosophers ignore or underestimate the contribution of social and other environmental factors to the limitations faced by people with disabilities.
In contrast, the social model explains the characteristic features of disability in terms of a relation between an individual and her social environment: the exclusion of people with certain physical and mental characteristics, or “impairments”, from major domains of social life. Their exclusion is manifested not only in deliberate segregation, but in a built environment and organized social activity that preclude or restrict the participation of people seen or labeled as having disabilities. A variety of social models are embraced by disability scholars and activists in and outside of philosophy. The “British social model” associated with the Union of the Physically Impaired against Segregation (UPIAS 1976) appears to deny any causal role to impairment in disability:
In our view, it is society which disables physically impaired people. Disability is something imposed on top of our impairments by the way we are unnecessarily isolated and excluded from full participation in society. Disabled people are therefore an oppressed group in society. Disability [is] the disadvantage or restriction of activity caused by a contemporary social organization which takes no or little account of people who have physical impairments and thus excludes them from participation in the mainstream of social activities.
Two features of this influential statement are worth noting, although we will only discuss the second at length. First, it limits itself to physical impairments; second, it contrasts impairments , individual characteristics or conditions, with disabilities , disadvantages imposed by society on those with impairments. The first feature inaugurates a long tradition in disability activism and scholarship of focusing exclusively on “physical” disability, to the neglect, if not the exclusion, of intellectual, psychiatric, and other “mental” disabilities. Both scholars and activists have long criticized, and sought to broaden, this narrow focus, and even those philosophers who continue to focus on physical disability recognize that adequate models and definitions must include mental disabilities as well. In the rest of this entry, we will not distinguish between the two types of disability except when it is relevant to a particular model or definition; we will note when an account is limited to physical disabilities or criticizes other accounts for that limitation.
The second feature, the distinction between impairment and disability, will be more central to our discussion. It is through those terms that the medical and social models have been distinguished, and it is this “anatomy” of disability that several recent philosophical definitions have rejected or significantly modified.
Implicit in the UPIAS understanding of disability are two ways that society imposes limitations on disabled people, corresponding to two distinct strands that might be a part of any social model. When the UPIAS claims that society “excludes” people with impairments, this suggests the minority group model , which sees people with impairments as a minority population subject to stigmatization and exclusion. On this view, the main reason people with disabilities encounter hardship is because they suffer discrimination along the same lines as racial or ethnic minorities. Accordingly, civil rights protections and anti-discrimination laws are the proper responses to disability (e.g., Hahn 1987 [1997] and Oliver 1990). Perhaps the most familiar expression of the minority-group model is found in the preamble to the Americans with Disabilities Act (ADA), which describes people with disabilities as “a discrete and insular minority”—an explicit invocation of the legal characterization of racial minorities.
The UPIAS also asserts that “contemporary social organization” fails to “take into account” people with disabilities. This suggests the human variation model, according to which many of the challenges faced by disabled people do not result from their deliberate exclusion, but from a mismatch between their characteristics and the physical and social environment. On this view, disability is
an extension of the variability in physical and mental attributes beyond the present—but not the potential—ability of social institutions to routinely respond. (Scotch & Schriner 1997)
This view of disabilities as the result of human variations is closely related to the view that disability is a universal human condition (Zola 1989) or shared human identity (L. Davis 2002: Ch. 1). The claim that disability is universal can be taken as nothing more than a prediction that we will all acquire familiar disabilities at some point in our lives. But that claim is better construed as one about the nature of disability; as maintaining that all human beings have physical or mental variations that can become a source of vulnerability or disadvantage in some settings.
These two versions of the social model are not incompatible, differing mainly in emphasis. The discrimination stressed by the minority group model generally leads to, and is expressed in, the societal failure to accommodate people with various differences. In some contexts, it is appropriate to analogize people with disabilities to racial or other minorities; in others, it is important to reject a dichotomy between disability and normality and treat impairments as continuous variations. If one goal of social policy is to remove discrimination and its enduring disadvantages, another is to encompass the full range of human variation in the design of the physical environment and social practices.
Although the social model, in one version or another, is now the dominant legislative, social-science, and humanities paradigm for understanding disability, stronger versions of it – particularly the British Social Model exemplified by UPIAS – have been subject to extensive criticism. Some argue that an adequate conceptualization of disability requires a recognition of impairments as an objective basis for classification, to distinguish disability discrimination from other types of discrimination (Bickenbach 1993). Several critics argue that extreme versions of the model implausibly deny or understate the role of impairment itself as a source of disadvantage (Anastasiou & Kauffman 2013; Terzi, 2004, 2009; Shakespeare 2006). Others, however, contend that this criticism is misplaced, because the British Social Model does not deny the importance of impairments but rather seeks to restrict the application of the term “disability” to social exclusion and oppression (Beaudry 2016).
Another objection is that the social as well as the medical model both rest on a false dichotomy between biological impairments and social limitations. There are two versions of this objection. One maintains that disability is a complex phenomenon, in which biological impairment and social exclusion are deeply interwoven and difficult to tease apart (Martiny 2015; Anastasiou & Kauffman 2013). The other version of this objection rejects the treatment of impairment as a (strictly) biological phenomenon. “Impairment”, the argument goes, is no less a social construction than the barriers faced by people so classified (more on this below). Claims that there is a stable biomedical basis for classifying a variation as an impairment are called into question by shifting classifications; by the “medicalization” of some conditions (shyness) and “demedicalization” of others (homosexuality). Moreover, the social environment appears to play a significant role in identifying and, arguably, in constituting some impairments (dyslexia) (Cole 2007; Shakespeare 2006; L. Davis 2002: Ch 1; Tremain, 2001, 2017; Amundson 2000). What counts as an impairment may depend on which variations appear to be disadvantageous in familiar or salient environments, or on which variations are subject to social prejudice: Less-than-average height may be more readily classified as an impairment than greater-than-average height because the former is more often disadvantageous in environments designed for people of average height, or because it is generally seen as less desirable. For such reasons, it is difficult to establish the objectivity of the impairment classification by appeal to a clear and undisputed biomedical norm. Amundson (2000), indeed, goes so far as to deny that there is any biological basis for a concept of functional normality—a claim emphatically rejected by Boorse (2010).
The debate between the medical and social model about the source of the disadvantages disabled people experience has dominated academic discourse about disability since the 1970s. More recently, however, disability activists and disabled scholars have questioned the apparent shared assumption of both models, that disability is fundamentally a matter of disadvantage, exclusion, or functional limitation. This to take a (partly) different view on what an account of disability should explain; a view consistent in principle with either a more medical or more social view of what does the explaining. The affirmative model of disability and impairment, as articulated by John Swain and Sally French (2000), holds that disability is not in the first instance a problem—not simply or solely a “personal tragedy”, and implicitly, not simply or solely a social injustice either. Rather, disability is a different way of living in and experiencing the world, one not characterized by its disadvantages any more than its advantages.
Note that this is not a claim about what causally explains disability; rather, it is a claim about what aspects of the phenomena of disability should serve as the object of explanation in social scientific theories of disability. As such, the affirmational model is prima facie consistent with either the medical or the social model, and indeed tends to draw on considerations from both. The diverse mix of advantages and disadvantages that characterize life with disability can derive from biological factors, social factors, or interactions between the two. On the side of advantage, a person with a disability like blindness might celebrate the increased attention sightlessness saves for hearing and other senses as well as the solidarity they experience with other disabled people as they fight together against ableism and for social justice. On the side of disadvantage, the affirmational model will point to the considerations some would regard as personal tragedies as, instead, a combination of purely functional challenges to be overcome, and conditions of social exclusion that can make life harder without thereby making it any less valuable or worth living.
Still: though logically independent of claims about the evaluative import of disability, the medical and social models suggest different views about the impact of disability on well-being, and different views about how disability is relevant to reproductive decisions, medical interventions, and social policy. The affirmational model is likely to be more in sympathy with social than medical models here. Those who accept a social model of disability regard the association between disability and well-being as highly contingent, mediated by a variety of environmental and social factors (Campbell & Stramondo 2017). They also tend to question conceptions of well-being that give a central role to the possession or exercise of the standard array of physical and mental functions, as those conceptions imply, or are often taken to imply, that well-being is precluded or diminished merely by the absence or limitation of those functions (see entry disability: health, well-being, and personal relationships ). As a result, they generally see the disadvantages of disability not only as externally caused, but as less formidable than they appear to people who view disability in largely biomedical terms. These differences are reflected in the conflicting assessments of life with disabilities found in the bioethics and public policy literature on the one hand, and disability scholarship on the other (contrast Brock 2005 with Goering 2008).
The different models of disability—and particularly, the medical and social models—have always been interpreted as favoring different responses to disability. The medical model appears to support the correction of the biological condition (or some form of compensation when that is impractical); the minority group model appears to favor measures to eliminate exclusionary practices or at least recognize their injustice; the human variation model appears to favor reconstruction of the physical and social environment to take into account a wider range of differences in human structure and function (measures that could in turn make the social environment less exclusionary).
But claims about the causal explanation of disadvantage do not always yield straightforward prescriptions for their remediation (Wasserman 2001; Samaha 2007; Barclay 2018). In some cases, medical or surgical “correction” may be the most effective way to escape discrimination; if correction is not appropriate, that is because it reinforces discriminatory attitudes and practices, not because it is discriminatory per se . Even an affirmational model does not straightforwardly imply that we should change society rather than disabled bodies: that disabled people have reason to be proud of their disabilities and/or impairments does not immediately entail claims in justice on the rest of us to incur the costs of accommodating these differences. This is to be expected: the proper response to the disadvantages associated with disability depends not only on causal attributions and prudential evaluations, the domains of the three “models”, but also on moral judgments about responsibility, respect, justice.
This is not to say that these causal attributions, much less prudential judgments, are morally irrelevant: to the extent that social causation of disability disadvantage makes social institutions morally responsible for the limitations disabled people face, it may be unfair and disrespectful for society to ask disabled people to change themselves rather than changing itself to be more inclusive (Aas 2020). Moreover, “correcting” disability may (as the affirmational model reminds) us involve destroying valuable forms of life and reducing the vibrant diversity of human embodiment; or it may not do not enough to counterbalance the benefits of uniformity (Garland-Thomson 2012). Contra the sense that the social, medical, and affirmational models each come bundled with obvious policy consequences, it seems clear on reflection that there is much yet to do to understand just what these different explanations of disability imply as to how we should respond to it.
2.Definitions of Disability
Until relatively recently, there was little independent philosophical discussion of definitions of disability. Instead, philosophers focused primarily on developing and interpreting legal and regulatory definition needed to implement disability policy. The legal definitions, in turn, were heavily influenced by the two-part “anatomy”—impairment and social response—of the social model of disability, which was developed by activists seeking to influence legislation and policy.
Thus, two familiar features are shared by most official definitions of disability, such as those in the World Health Organization (1980, 2001), the Disability Discrimination Act (UK), and the Americans with Disabilities Act (United States): (i) a physical or mental characteristic labeled or perceived as an impairment or dysfunction and (ii) some personal or social limitation associated with that impairment. Impairments are generally seen as traits of the individual that he or she cannot readily alter. Just what makes a condition a trait or attribute of an individual is obscure and debatable, but there seems to be agreement on clear cases. Thus, poverty is not seen as an impairment, however disabling it may be, nor is tasteless clothing, even if it is a manifestation of impaired fashion-sense rather than scarce income. On the other hand, diseases are generally classified as impairments, even though they are often neither permanent nor static conditions. Diseases that are especially transient, however, such as the flu and the measles, do not normally count as impairments.
As in early philosophical debates about competing models, the most controversial issue in defining disability is the relationship between these two features. At one extreme are definitions that imply, or are read to imply, that biological impairments are the sole causes of limitation. The definitions in the World Health Organization’s 1980 International Classification of Impairment, Disability, and Handicap, and the Disability Discrimination Act (UK) have been interpreted this way. At the other extreme are definitions that restrict the limitations faced by disabled people (as such) solely to “contemporary social organization”, such as the definition given by the Union of the Physically Impaired Against Segregation (UPIAS 1976). In between are definitions which assert that individual impairment and the social environment are jointly sufficient causes of limitation. Perhaps the best-known example is the WHO’s International Classification of Functioning, Disability and Health (World Health Organization 2001, referred to as ICF), which emphasizes that disability is a “dynamic interaction between health conditions and environmental and personal factors”.
Through much of the first two decades of this century, philosophers were largely content with this definitional approach to disability as a relationship or interaction, disagreeing primarily on the comparative contribution of the two elements and the policy relevance of their contributions. As noted in the last section, dissenters mainly focused on the characterization of one or both elements, as, e.g., on the first as social vs. biological, rather than on the “anatomy” itself. More recently, however, there has been some movement away from reliance on these two-part approaches to defining disability (e.g., Barnes 2016, and much of the literature responding). One reason may be that in most settings, we do not think of or refer to disabilities as relationships or interactions, but as individual somatic or psychic traits, states or conditions (including absences and deficiencies). These commonsense referents are hard to find in, for example, the multifactorial charts by which the ICF illustrates its definition of disability as a complex interaction of health conditions with environmental, social, and personal factors.
Some might argue that ordinary usage is ideological, shaped by false failure to be conscious of the insights of social and interactionist models. But defining “disability” in rough conformity to ordinary usage hardly implies that its referents are selected by biomedical criteria, let alone that the traits selected cause the disadvantages faced by their bearers or dictate the appropriate social response to those disadvantages. Rather, this view on what “disability” and “people with disabilities” refer to is compatible with a wide variety of positions on how those referents are picked out: e.g., by biomedical criteria; by the rules of a civil-rights movement; by the assumptions of the dominant ideology about bodily dysfunction; or by the demands of justice. The extent to which what counts as a disability, or a person with a disability, varies with context will depend on the account adopted; on biomedical accounts, the extension of “disability” will be as stable as human biology; on other accounts, it will change with changing social norms, economic needs, or political developments. Further, on some accounts, the referents will have common features, identifiable by inspection; on others, what they have in common can only be understood in terms of an ideology or a theory of justice.
After discussing several types of accounts, we will address the claim, inspired by the diversity of traits and conditions they pick out, that “disability” has no core meaning, and that it may be futile and distracting to search for one.
2.2 Philosophical Definitions of Disability
Outside of legal and policy interpretation, philosophers have made a number of claims about the definition of “disability”—at first, mostly only in passing, during discussion of other matters, like “disease” and “health”; later as an increasingly important philosophical topic in its own right.
Given the pervasiveness of medical models of disability in the culture, one would think that at least some recent philosophers would defend a view of disability on which it is defined in terms of pathology or departure from normal functioning (see entry on concepts of health and disease ). So far we can tell, however, no one has done so explicitly, in print. Christopher Boorse, perhaps, comes closest, when he says:
at first sight, one expects disability […] to consist of a pathological condition severe enough to have certain morally and legally important effects. (Boorse 2010: 60–61)
Though Boorse only broaches the possibility of such a definition, without defending, his broader views about health and disease may seem to support this approach. If, as Boorse argues there is a good naturalistic sense of “pathology” as (statistically) downward departure from species-typical functioning, then that notion can be inputted into our moral and political thinking to produce a definition of disability on the following pattern:
S is disabled, in a context C , iff
- S has a pathology—that is, some part of their body performs its normal function at statistically subtypical levels,
- In C , that pathology causes effects that make a difference, of kind D , to how S ought legally or morally to be treated
To fully develop this view, of course, one would need to say what sort of moral/legal difference pathology is supposed to make—not just any difference will do, since it would not follow from the fact, say, that everyone has a legal or moral right to treatment for transient injuries or diseases that all these conditions are disabilities. Note also that, though this view mentions the medical concept of pathology, as a definition of disability it does not entail a medical model, or indeed even the denial of the affirmational model. The medical/social debate will turn on the extent to which it is pathology itself that makes a moral difference, rather than pathology in combination with social factors. The affirmational model debate will turn on just which effects are definitive of disability; if these are all negative or harmful, it will be harder to understand disability as something to be proud of. But the bare fact that disability arises from pathology, on this definition, does not necessarily preclude pride in it, given Boorse’s normatively neutral definition of pathology.
That said, few philosophers seem inclined to defend this way of defining disability. Many philosophers are skeptical of the analytic division between facts about bodily function and social and ethical norms, arguing that there is no way to define disease or pathology independent of “normative” considerations (Wakefield 1992; Kingma 2007; entry on concepts of health and disease ). Those sympathetic to the claims of the disability may have more specific qualms, as well. Those attracted to the “human variation” version of the social model may be skeptical that all of the bodily difference that make for disability are statistically atypical in the required way, e.g., very common or universal conditions like age-related hearing loss or atherosclerosis. Those who tend more to a “minority group” model will tend to see the bodily differences that matter to disability as perceived or represented difference, rather than actual difference. And anyone with any sympathy to the social model at all will tend to think that, as-so-far stated, this definition puts its philosophical precision in the wrong place: that it is at least as important to understand what social, moral, and legal effects characterize disability as to understand which sorts of causes these effects must have to count as “disabling”.
Kahane and Savulescu (2009; Savulescu & Kahane 2011) propose a reforming definition of disability that promises to avoid potentially problematic references to pathology. Their basic idea is that a disability is a (broadly) bodily condition that makes its bearer worse off. To wit:
“disability” should refer to any stable physical or psychological property of subject S that leads to a significant reduction of S ’s level of wellbeing in circumstances C , excluding the effect that this condition has on wellbeing that is due to prejudice against S by members of S ’s society. (Savulescu & Kahane 2011: 45.)
This view adopts certain insights of the social model: in particular in holding that disability is relative to circumstance and in downplaying the role of pathology or biological abnormality in defining disability (note there is no reference to “impairment”, not even records or appearance of impairment).
In other ways, however, it seems to be significantly out of step with both the letter and the spirit of social models of disability. On this definition, a condition which is only harmful in virtue of social prejudice would not be a disability. Even the softer social model implicit in the Americans with Disabilities Act allows that some people are disabled solely in virtue of being “regarded as” impaired; those in that group who experience discrimination as a result would still not be “disabled” on Kahane and Savulescu’s view. Just how out of step this judgment is with the usual commitments of the social model, may depend on the relative importance it places on prejudice as compared to other factors in producing disability disadvantage. A social model that cleaves closely to a “minority group” understanding of ableist injustice may find that this definition excludes the paradigm cases of disability, people who experience gross or net reductions in advantage due to prejudicial phenomenon like stigma and intentional exclusion. A “human variation” account of most disability disadvantage would see more possibility for people to be disadvantaged by non-prejudicial mismatches between atypical bodies and societies built for typicality, since this account will say that many of the welfare costs experienced by people with atypical bodies are not a result of prejudicial attitudes per se , even if they often reflect structurally unjust failures of inclusion.
It should be even more clear that the affirmational model of disability is in substantial tension with this harm-requiring definition of disability. Granted, affirmation of disability may not be formally inconsistent with defining it in terms of harm, since it is possible in principle to take pride in or otherwise be glad about something that leads to a reduction in our well-being (since there are things in life that matter, besides our own well-being). But affirmational models generally hold that being disabled is not always or in general a cost to our well-being (Swain & French 2000; Barnes 2016). This would be a conceptual falsehood, on the welfarist view: something which is not a cost to well-being in some context is simply not a disability.
Are these decisive problems for defining disability in terms of welfare? Much depends here on what we intend to do with definitions of disability. If the goal is to capture ordinary usage, a welfarist view may be on the right track. It might account, for instance, for the broad appeal of slogans like “deafness is not a disability” and euphemisms like “differently abled”; these expressions, on this view, would be ways of emphasizing some of the substantive evaluative intuitions behind the affirmative model, that most conditions we call disabilities are not so bad absent prejudice. That said, disability scholars and activists have tended to be skeptical of such expressions, on the grounds that they undermine efforts to see disabled people as a politically salient group with similar experience of ableism and strong reason to work together for justice, rather than to simply commiserate. If a definition of disability should advocate in favor of usages that produce a better or more just world, this might be a reason to reject Kahane and Savulescu’s view, in favor of one that allows people to be disabled due to prejudice and/or in the absence of harms to well-being. Or at least, this will be so if the social and/or affirmational models of disability have the moral and political advantages proponents advertise for them.
Most philosophers who have considered the definition of disability in recent years have written in sympathy with either or both of the social or affirmational model of disability.
Elizabeth Barnes’s critique of definitional claims implicit in the social model has been a signal moment in the recent debate. Barnes is concerned that thinking of disability as a stigmatizing, oppressive, and exclusionary response to bodily difference does not distinguish disability from other properties grounded in responses to the body, like (on many accounts) race, gender, and sexual orientation identities.
Barnes develops an alternative view which still defines disability as a social property—but in a way that fits the affirmational model better than the definitions suggested by classic social models, doing away with the distinction between disability and impairment and making no direct reference whatsoever to injustice or disadvantage. Barnes (2016) proposes to define disability in terms of the judgments of disabled people themselves, not society as a whole. To wit, S is (physically) disabled if and only if:
- S is in some bodily state x ; [such that]
- The rules for making judgments about solidarity employed by the disability rights movement classify x in context C as among the physical conditions that they are seeking to promote justice for.
This makes who is disabled a social construction—dependent on the attitudes and commitments of a particular, self-identified group of people in contemporary society, the “disability rights movement”, composed of self-identified disabled and nondisabled members. It thus raises the concern that a disability movement might seek justice for the wrong people. Couldn’t some of those people complain that they should be included in the aims of that movement, precisely, because they are disabled? Barnes responds in two ways. The first is to note that she appeals to the rules for judgment-making, rather than judgments themselves; some people might not actually be included in the disability rights movement—say, because of internal prejudices on the part of those within the movement—but if this is inconsistent with the reasons for including others, then the excluded people will count as disabled too, on Barnes’ account. Still one might ask, what if the rules themselves were bad rules, wrongly but consistently excluding some people form the ambit of the struggle against ableism? Barnes, in response to this, rigidifies, insisting that we judge disability relative to the rules of the actual disability movement, even when we are imagining situations where that movement should use different rules than it actually does.
Some are not convinced by this last reply. For it can seem to give too much weight to judgments of the actual disability rights movement. As Jenkins and Webster point out, “rigidifying” to the actual world in this way means that imagining a world with a different disability rights movement isn’t imagining a world with different disabled people. But what if the disability rights movement is different there because social conditions are different, warranting a different set of rules for determining which people with pathologized bodily difference to seek justice for? And indeed isn’t there a sense in which “there” could be “here”? That is, couldn’t the disability right movement as it actually is, use rules that even when consistently applied lead it to seek justice for the wrong people (Wasserman 2018; Howard & Aas 2018; Lim 2018)?
This last concern can be generalized. Chong-min Lim, responding to Barnes, questions why the disability movement alone should have the authority to constitute disability. Where, we might ask, does this leave the experience of disabled people not part of the movement, or of those caregivers and/or non-disabled loved ones who advocate for them? And couldn’t the disability movement be overinclusive too, in principle, attempting to expand solidarity beyond what makes sense morally or politically. To address this problem (and in the process, expand the account to cover cognitive and other “non-physical” disabilities), Lim proposes that we make the following modification to Barnes’ account:
S , is disabled in context, C , if and only if:
- S is in some state, x ;
- x is constitutive, in C , of some constraint on S ’s legitimate interests;
- x is regarded, in C , as the subject of legitimate medical interest;
- the rules employed by the disability rights movement classify x in C as among the traits that they are seeking to promote progress and change for. (Lim 2018: 987)
Relative to Barnes, II and III are new restrictions, while IV is a substantially broadened version of the main clause of Barnes’ approach—in effect, broadening the relevant goals to include any improvement in the lives of putatively disabled people, whether that comes from social change or bodily transformation. Relatedly, III seems to bring back in medicalization—though now constrained by the requirement that the medical interest in question be “legitimate”, meaning, not apt in the traditional sense (not, concerned with pathology ) but rather just or right ; morally legitimate in light of whatever morally appropriate role medicine has to play in our society. Lim introduces these conditions to reflect the fact that expert communities outside of the disability rights movement have expertise relevant to constituting the disability population; parents or caregivers, even those not part of the movement itself, may have insight into whether and how a condition affects legitimate interests, while physicians will have important (though not exclusive) knowledge of which limitations on function are legitimately subject to medical interest.
The (intended) effect of Lim’s modifications, then, would be to limit the authority of the particular political judgments of the actual disability rights movement in determining who is disabled. This points to what may be a deeper problem for Barnes’ account, and the parts of Lim’s that follow her in making recognition by the rules that guide the disability movement determinative of disability. If the disability movement ought to adopt rules that pick out a certain group, isn’t that precisely because that group shares some other property, that makes that choice reasonable? That is, isn’t there something that those the disability rights movement share, that explains why they ought to seek justice in solidarity together? Wouldn’t that thing, whatever it is, make a better candidate definition of disability? To put the question for Lim’s account in particular: why would we want to deny that a condition is a disability, it if were a medically interesting constraint on legitimate interests, but not recognized as such by the rules of the disability rights movement?
Howard and Aas (2018) respond to Barnes in a different way, developing a definition that harkens back to the classic social model of disability. Building on the work of Sally Haslanger (2000) on gender and race, they define disability classically as a certain sort of social response to impairment. On their view, person S is disabled in a context C , iff
- S is in some bodily or psychological state x [such that]
- x is regularly assumed in the ideology in C to involve an impairment: a dysfunctional bodily state that limits a major life activity, and
- in the dominant ideology of C , that someone in x has an impairment explains why they can be appropriately pitied, stigmatized, and excluded from socially valued activities and statuses.
- The fact that S is in this state plays a role in S ’s systemic disadvantage: that is, (i)–(iii) actually explains why S is involuntarily excluded from certain valued activities or relegated to a marginal status along some significant social dimension. (2018: 1128–1129)
Impairment is critical on this analysis. Disability is distinct from other bodily-based social categories on this definition precisely because it is a response, of a certain distinctive sort, to social perception about bodily properties, namely impairment . Race, gender, and orientation identity would be different (thought possibly overlapping) responses to different (again, possibly overlapping) bodily properties. Howard and Aas do not, however, defend the biological reality of impairment; it suffices for their account that society itself employs some notion of biological abnormality or insufficiency, saying with the classic social model that disability is a matter of being classified as impaired, and excluded on that basis.
Barnes (2018) responds that, because of this last feature, this account does not after all give sufficiently central place to bodily difference. In particular, she thinks it makes it hard to see how the bodily differences characteristic of disability could be, as the affirmation model has it, something to be proud of. They are, after all, picked out negatively, by reference to disadvantage and social exclusion. Bodily features picked out for their role in the struggle for disability justice seem to be a better candidate source of joy, identification, and pride. The success of Barnes’ response depends on how exactly disability pride is supposed to work, and on how exactly definitions like these are supposed to serve the interests of the struggle against injustice. Among other things, reflection on related cases involving racialized body features suggests that it is possible to take pride in something that others respond to in oppressive and stigmatizing ways. On this understanding, the pride is not in the oppression, but in the oppression-triggering feature itself or in a skillful or solidaristic response to oppression.
Jenkins and Webster (2021) propose a different sort of social-construct definition of disability—or actually, three different but closely related definitions. Like Barnes, Howard, and Aas, they are interested in understanding what bodily differences are centrally relevant to disability. But they cleave closer to the human variation model than the minority group model in understanding these differences. Their key notion is what they call marginalized functioning : having a body that does not work in the way that our socially constructed world expects. Each of their three definitions of disability presuppose this notion; to wit:
MF1 : A subject S is [physically] disabled if they have marginalized functioning relative to a context, C , where this is the case iff:
- there is a set of social norms N , comprising \(n_1,\) \(n_2,\) …\(n_n,\) each of which serves as a default for the purposes of constructing common social environments and structuring common social interactions in C ; and
- there is some norm in N , \(n_x,\) such that S cannot physically function in a way that satisfies it. (2021: 8)
It might seem that this account, and indeed Howard and Aas’s, implies that there could be no disability in a just society. Though this is a classic claim of the traditional British social model of disability (UPIAS 1976), some find it implausible. Note, however, that neither of these views in fact implies the impossibility of disability in a just society (even if their language sometimes suggests it). For neither view, in itself, implies that the social responses that constitute most disabled people as such are necessarily unjust (though surely all four authors would agree that in the actual world, they usually are). If it is morally legitimate to set society up in a way that is designed for the functioning of most but not all its members—and it may well be, given how costly it would be to get anywhere near complete and comprehensive inclusion (Barclay 2018)—then some forms of functioning could be marginalized or be a source of disadvantage, even in a just society. And, thus, those that function in those marginalized ways, could be disabled.
A more significant prima facie concern for MF1 is that it seems to include amongst the disabled people with merely transitory mismatch between body and society—say, someone who broke one or both arms, and therefore cannot open doors or otherwise do what society expects people to be, physically, able to do. These people do not normally identify and are not normally identified as disabled. To capture this, Jenkins and Webster propose that we might move, simply, to:
MF2: someone is disabled in a context if and only if they have lasting marginalized functioning in that context; OR
MF3: someone is disabled in a context if and only if they experience disability-characteristic oppression because they have marginalized functioning in that context
MF2 solves the problem of temporary conditions by stipulation. This may or may not be good enough here, depending on whether we think temporary conditions (e.g., post-concussion syndrome or pregnancy) can be disabilities. MF3 faces some of the same problems as other social-model-inspired definitions—particularly, that it seems to define disability in terms of a kind of oppression, and therefore in terms of something bad, something that is therefore (arguably) difficult to be proud of or happy about. Further, by requiring that oppression be caused by functioning that actually fails to fit going norms and expectations, it does not clearly classify as disabled people who are disadvantaged by false perceptions regarding their bodily differences—again, failing to follow the ADA in its well-considered inclusion of people “regarded as”, but not, impaired, in its definition of disability (Francis 2018). It remains to be seen whether the advantages of this definition are great enough to justify excluding such “regarded” as people as disabled.
In their influential book From Chance to Choice , Buchanan, Brock, Daniels, and Wikler (2000) propose the following definition, meant as an explication of the legal and policy decisions considered above.
To have a disability is to be unable to perform some significant range of tasks or functions that individuals in someone’s reference group (e.g., adults) are ordinarily able to do, at least under favorable conditions, where the inability is not due to simple and easily corrigible ignorance or to lack of the tools or means ordinarily available for performing such tasks or functions. (2000: 286)
This defines disability colloquially, in terms of ability; disability is, roughly, an unusual inability. Barnes and others object, however, that this definition is too broad. It seems to make it the case, for instance, that someone who cannot “roll their tongue” or do mental subtraction is disabled; since most people can do this under favorable conditions. Conversely, this sort of view also seems to undergenerate disabilities, since some (fibromyalgia or depression for instance), only make it more difficult to do things, without making any particular task or function straightforwardly unachievable. And it is not entirely clear how this account avoids the obviously problematic implication that identity categories like race, gender, and sexual orientation imply disability; someone subject to social prejudice in virtue of their gender or the color of their skin might be, for that reason, unable to do things others can do.
Alex Gregory (2020) takes a different approach to defining disability in terms of inability:
The Inability Theory: To be disabled is to be less able to do something than is typical, where this degree of inability is partly explained by features of your body that are atypical. (2020: 26)
This definition of disability brings the body into the definition, but it is meant to be neutral between more-medical and more-social ways of seeing disability. “Atypical” features need not be “abnormal” in a medicalizing sense; they are simply different, not necessarily worse. To say that an inability that comes to disability must be at least partly explained by bodily features is consistent, both, with saying that it is entirely explained by them (a la the medical model) and that it is also partly explained by social factors. This in itself rejects the medical model as a general claim, as well as the less nuanced statements of the social model, that would definitionally exclude non-social inabilities from the ambit of “disability”.
The initial statement of the Inability Theory would still seem to be overinclusive; someone who cannot get a good job because of the color of their skin, or marry the person they love because of their sexual orientation, has an atypical inability explained by an atypical bodily feature. To rule these cases out, Gregory moves to:
The Final Inability Theory: To be disabled is to be less able to do something than is typical, where this degree of inability (1) is partly explained by features of your body that are atypical, and (2) is not explained by anyone’s attitudes toward those bodily features. (2020: 33)
This does plausibly avoid the problem of classifying sexual and racialized minorities at least as disabled; any inability engendered by color of skin is explained entirely by prejudicial attitudes. (Or so it may seem; more below). But in the process it also raises a recurring problem—where an atypical feature is only inability-generating because of attitudes specifically about whether it is inability-generating . If people think that people with, say, Down syndrome, cannot benefit from education, they will not be educated; when they do not develop the skills they could have developed, that lack of skill is, then, explained by a combination of atypical bodily features and attitudes towards those features. It can seem plausible to say, with the ADA, that discrimination rooted in a pathologized understanding of a trait is a kind of disability discrimination.
Moreover, this analysis also raises some of the same concerns as those Barnes and others pressed against Buchanan et alia ’s explication of disability as biologically abnormal limitation. For here even more than there it seemed like not every limitation on ability, not even every one explained by atypicality or abnormality, is a disability properly-so-called. Gregory, however, has a novel response here—insisting that these are, really, disabilities, but just not normally worth calling attention to as “disabilities”, since the aptness of this ascription in conversational context depends on the significance of the abilities at issue.
This proposal raises other problems, however.. Recall race and sexual orientation. A person with light-colored skin cannot work in even relatively moderate sun all day without getting a sunburn. Someone with exclusively same-sex orientation cannot have procreative sex with someone for whom they have romantic and sexual feelings. These are inabilities explained by bodily difference, not by attitudes, and they are not insignificant or trivial ones: yet it seems they are not disabilities, not even a little bit.
Why not? The social constructionist views considered above would give one kind of answer—pointing to the facts that (depending on the view):
- the disability rights movement is rationally unconcerned with properties like race and orientation; or
- that race and orientation are not targeted by ableist ideology for exclusion and stigmatization; or
- that our actual social norms do not marginalize these configurations of bodily function, in the way they marginalize paradigm impairments.
An alternative, more positive approach, which remains focused squarely on ability, would hold that these inabilities, like the minor inabilities considered above, are not relevant to disability because their absence does not place claims on others, in justice. To wit, Jessica Begon (2021)
Thus, I define disability as the restriction in the ability to perform those tasks human beings are entitled to be able to perform as a matter of justice, as the result of the interaction between an individual’s impairment, their social and political context, and the resources they have available to them. (2021: 936–937)
It turns out that by impairment Begon simply means “atypical or unusual functioning”, not pathological or life-limiting functioning; so, this account is actually structurally more similar to Gregory’s than to Buchanan et alia. The difference is that the specific absence of ability that constitutes a disability is the atypicality-caused absence of abilities we ought to have , or anyway that our societies ought to provide for us.
This account has a natural response to the problems of non-disability inabilities. No one is entitled to roll their tongue (at least in any social environment remotely like our own); thus, nobody is disabled because they cannot do so. Nor, in most circumstances, are we entitled to sit unprotected all day in the sun without paying the consequences. We might be entitled to protection by sunscreen, or to the opportunity to escape the sun, but we are not entitled to have the ability to withstand the sun if we choose to forgo these protections. Similarly, it seems plausible to deny that anyone is entitled to procreate sexually with their romantic partner; there may be entitlements to become a parent, perhaps even a genetic parent, but they need not be realized in this way. Thus, Begon’s account appears at first glance not to overgenerate disabilities, as other inability-based accounts seem to.
That said, the account still faces some of the problems we see with other ability-limitation-based accounts. The non-pathologizing sense of impairment as “functional difference” may not in the end be specific enough to distinguish disability from other kinds of unjust absence of ability. Begon addresses this in the case of sex difference, arguing—in effect, with Boorse—that differences in the “reference class” or appropriate functional norms applying to males and females of the species make for differences in what counts as an impairment between males and females. So, for instance, an inability to get a good-paying job resulting from possession of the capacity to menstruate is not a disability, because that capacity is not atypical for female human beings . Such a way to address the problem may not cover all forms of oppression since much oppression seems to be evoked by differences that are functional in some sense—sexual orientation relates to the function of our dispositions to sexual attraction; absence of athletic ability (within the normal range) to the function of the musculature; even pigmentation, to the function of the epidermis in protecting the organism from the environment.
Begon’s view could avoid classifying inabilities down to these differences by further multiplication of “reference class”, so that, say, being unable to get a job because you are gay is not a disability because gay people function typically “for gay people”. But as Elselijn Kingma has argued, in response to similar maneuvers in the health literature, this kind of specificity seems problematically arbitrary—in the limit, threatening to trivialize the relevant notion of “functional typicality” (Kingma 2007). These concerns seem to press back in the direction of Lim’s restriction of disability to responses to “medically significant interests”, or Howard and Aas’s definition in terms of traits perceived or represented as functional deficits in the reigning biomedical ideology.
There are also questions about how we are to understand the set of entitlements relevant to determining when the absence of ability is unjust. Begon discusses these issues only briefly (2021: 954, n30); a more fully developed version of the view would have to do more. It seems important to abstract from resource constraints, since we would not want to say that someone is only disabled if habilitating them is cost-effective relative to other priorities justice gives us, given what resources we happen to have. But this abstraction threatens to make too many of us disabled, since justice might, absent resource constraints, give us powerful reasons to enable one another to do all sorts of things—to give those of below-average height the ability to dunk a basketball, say; or to give women well-past childbearing age the ability to conceive and gestate children. Perhaps we should do these things in response to these functional atypicalities; that does not make people disabled, until we are rich enough to do them.
Two sorts of skeptical responses have greeted the effort to define disabilities as individual traits, conditions, or functions, selected by some set of rules or criteria. The first critique is inspired by the work of Michael Foucault on biopower as a form of control exercised by modern states over the bodies of their populations (Tremain 2017). This critique argues that to focus on individual characteristics in defining disability is to miss the forest for the trees. “Disability” refers not to a set of individual characteristics, or to a concept that encompasses such a set, but to a mechanism that identifies various types of individual characteristics for the purpose of social control. Notably, Shelley Tremain analyzes disability as a mechanism constructed and maintained by laws, informal norms, cultural understandings and other exercises of biopower. Impairments and disabilities only exist within this culturally and historically contingent apparatus that arose in part as a means for people who saw themselves as “normal” to regulate those they labeled as “deviants”.
[D]isability is not a metaphysical substrate, a natural, biological category, or a characteristic that only certain individuals embody or possess, but rather is a historically contingent network of force relations in which everyone is implicated and entangled and in relation to which everyone occupies a position. That is, to be disabled or non-disabled is to occupy a certain subject position within the productive constraints of the apparatus of disability…. (2017: 22).
At first glance, Tremain’s Foucauldian claim can seem to be talking past the interlocutors considered above; no more a distinctive analysis of disability to compete with the foregoing than was Foucault’s famous claim that “knowledge is power” a competitor to Plato’s or Goldman’s or Sosa’s analytic definitions of knowledge (see entry on the analysis of knowledge ). As in that case, however, a recognition of the role the concept of disability plays in reproducing unjust social conditions can cast doubt on reliability of the commonsense judgments and linguistic intuitions appealed to by rival analytic definitions. Such judgments and intuitions are, so the Foucauldian could argue, products of the apparatus, not an independent basis for assessing or understanding its assignment of positions. However, several of the analytic accounts discussed in the preceding action were developed with awareness of and due skepticism towards the ideological roots of prevailing convictions about disability and do not explain disability as a natural, biological category. It is unclear then, if a Foucauldian challenge could undermine the evidence used to develop these accounts.
The second critique, rather than dismiss the value of philosophical definitions, emphasizes their multiplicity, maintaining that different definitions are appropriate in different contexts and for different purposes. On this view, the problem with these definitions is that they see themselves as competitors in pursuing a goal that is both unattainable and undesirable: a single unified or core definition of disability:
Many philosophical disagreements about disability simply overlook the fact that the disputants are talking about different phenomena (impairment vs. oppression; care vs. justice; legal vs. extra-legal obligations, etc.). Some of those disagreements are more productively articulated as disagreements on how to handle the polysemy of disability. (Beaudry 2020: 5; see also Beaudry 2016).
Though certain ethical or political contexts might call for specifying or stipulating a definition, this view holds that we have little reason to think we can find, or should seek, a definition of “disability” as a general matter. We are unlikely to find one because these different definitions will have conceptual and practical advantages in different contexts; we should not seek one because adopting a canonical definition would foreclose our recognition of other characteristics and phenomena with moral and practical affinities to what we have decided to call “disabilities”. An open-ended approach, in contrast, “can create avenues for new kinds of emancipatory self-understandings” (Beaudry 2020: 13).
Beaudry acknowledges that even open-ended approaches have evidentiary constraints, but these constraints are far looser than any which a single definition, however nuanced and complex, would impose:
Disability remains a term that at least denotes or connotes “abnormal embodiments”, including phenomena entirely external to the bodies of “disabled persons” (such as prejudices directed at imagined abnormal embodiments or strictly cultural artifacts). It is a useful commonality between a constellation of discourses that relate to objects that are at least united by this family resemblance and may overlap or interact with each other, even though it is unlikely that a “master theory” would neatly choreograph all such interactions. (Beaudry 2020: 17)
This deflationary pluralism, however, arguably overlooks the value of continuing to seek a single unified or core definition of disability, however unlikely we are to agree on one. Most philosophers who have taken this tack do so not on the supposition that “disability” or even “impairment” are natural kinds—objective properties that legal and regulatory definitions ought to track. Rather, they are largely motivated by a belief that there is a set of personal experiences and social responses that people with disabilities have in common, and that ways of precisifying the meaning of “disability” and “impairment” are likely to work better than others for purposes of framing policies and building political movements to address the needs and claims of individuals those sharing such personal experiences and aimed at addressing the moral and political of this group.
Whether and to what extent the practical aims these various models of disability seek to serve are best accomplished by many separate contextual definitions, or one sophisticated one is, in the final analysis itself likely to be a difficult ethical, even political, question. Proponents of social constructionist, ameliorative views of disability, like proponents of similar views of race and gender, have tended to think that there are good practical reasons to define these notions broadly, to draw attention to forms of injustice that many experience, together, as a means for building larger and thus more powerful coalition to push for positive change. And they have, or anyway could, argue that the flexibility and inclusiveness pluralist call for can be accommodated by an open-minded and sensitive debate over just what this one solidaristic definition should or should not include. They might be right, or they might be wrong, but if they are wrong, it is not because the philosophical and political project of offering a unifying definition is a priori misguided.
- Aas, Sean, 2020, “Disability, Society, and Personal Transformation”, Journal of Moral Philosophy , 18(1): 49–74. doi:10.1163/17455243-bja10060
- Albrecht, Gary L., Katherine Seelman, and Michael Bury (eds.), 2001, Handbook of Disability Studies , Thousand Oaks, CA: SAGE Publications. doi:10.4135/9781412976251
- Altman, Barbara M., 2001, “Definitions, Models, Classifications, Schemes, and Applications”, in Albrecht, Seelman, and Bury 2001: 97–122. doi:10.4135/9781412976251.n4
- Amundson, Ron, 1992, “Disability, Handicap, and the Environment”, Journal of Social Philosophy , 23(1): 105–119. doi:10.1111/j.1467-9833.1992.tb00489.x
- –––, 2000, “Against Normal Function”, Studies in History and Philosophy of Science Part C: Studies in History and Philosophy of Biological and Biomedical Sciences , 31(1): 33–53. doi:10.1016/S1369-8486(99)00033-3
- Anastasiou, Dimitris and James M. Kauffman, 2013, “The Social Model of Disability: Dichotomy between Impairment and Disability”, Journal of Medicine and Philosophy , 38(4): 441–459. doi:10.1093/jmp/jht026
- Anderson, Elizabeth S., 1999, “What Is the Point of Equality?”, Ethics , 109(2): 287–337. doi:10.1086/233897
- Asch, Adrienne, 2006, “Appearance-Altering Surgery, Children’s Sense of Self, and Parental Love” Surgically Shaping Children: Technology Ethics, and the Pursuit of Normality , Erik Parens (ed.), Baltimore, MD: John Hopkins University Press, pp. 227–252.
- Asch, Adrienne and Michelle Fine, 1988, “Introduction: Beyond Pedestals”, in Women with Disabilities: Essays in Psychology, Culture, and Politics , Michelle Fine and Adrienne Asch (eds.), Philadelphia, PA: Temple University Press, pp. 1–37.
- Banks, Martha E. and Ellyn Kaschak (eds.), 2003, Women with Visible and Invisible Disabilities: Multiple Intersections, Multiple Issues, Multiple Therapies , New York: Haworth Press.
- Barclay, Linda, 2018, Disability with Dignity: Justice, Human Rights and Equal Status , New York: Routledge. doi:10.4324/9781351017114
- Barnes, Elizabeth, 2016, The Minority Body: A Theory of Disability , Oxford: Oxford University Press. doi:10.1093/acprof:oso/9780198732587.001.0001
- –––, 2018, “Against Impairment: Replies to Aas, Howard, and Francis”, Philosophical Studies , 175(5): 1151–1162. doi:10.1007/s11098-018-1075-x
- Basnett, Ian, 2001, “Health Care Professionals and Their Attitudes toward Decisions Affecting Disabled People”, in Albrecht, Seelman and Bury 2001: 450–467.
- Beaudry, Jonas-Sébastien, 2016, “Beyond (Models of) Disability?”, Journal of Medicine and Philosophy , 41(2): 210–228. doi:10.1093/jmp/jhv063
- –––, 2020 “Theoretical Strategies for Dedining Disabilities”, in The Oxford Hanbook of Philosophy and Disability , David Wasserman and Adam Cureon (eds.), Oxford: Oxford University Press.
- Begon, Jessica, 2021, “Disability: A Justice-Based Account”, Philosophical Studies , 178(3): 935–962. doi:10.1007/s11098-020-01466-3
- Bickenbach, Jerome Edmund, 1993, Physical Disability and Social Policy , Toronto and London: University of Toronto Press.
- Brock, Dan W., 2005, “Preventing Genetically Transmitted Disabilities While Respecting Persons with Disabilities”, in Quality of Life and Human Difference: Genetic Testing, Health Care, and Disability , David Wasserman, Jerome Bickenbach, and Robert Wachbroit (eds.), Cambridge: Cambridge University Press, pp. 67–100. doi:10.1017/CBO9780511614590.004
- Boorse, Christopher, 2010, “Disability and Medical Theory”, in Philosophical Reflections on Disability , D. Christopher Ralston and Justin Hubert Ho (eds.), (Philosophy and Medicine, 104), Dordrecht: Springer Netherlands, pp. 55–88. doi:10.1007/978-90-481-2477-0_4
- Brickner, Richard P., 1976, My Second Twenty Years: An Unexpected Life , New York: Basic Books.
- Buchanan, Allen, Dan W. Brock, Norman Daniels, and Daniel Wikler, 2000, From Chance to Choice: Genetics and Justice , Cambridge: Cambridge University Press. doi:10.1017/CBO9780511806940
- Campbell, Stephen M. and Joseph A. Stramondo, 2017, “The Complicated Relationship of Disability and Well-Being”, Kennedy Institute of Ethics Journal , 27(2): 151–184. doi:10.1353/ken.2017.0014
- Charlton, James I., 1998, Nothing About Us Without Us: Disability, Oppression and Empowerment , Berkeley, CA: University of California Press.
- Cole, Phillip, 2007, “The Body Politic: Theorising Disability and Impairment”, Journal of Applied Philosophy , 24(2): 169–176. doi:10.1111/j.1468-5930.2007.00369.x
- Cohen, G. A., 1993, “Equality of What? On Welfare, Goods, and Capabilities”, in The Quality of Life , Martha Nussbaum and Amartya Sen (eds.), Oxford: Clarendon Press, pp. 9–29. doi:10.1093/0198287976.003.0002
- Crawford, Danette and Joan M. Ostrove, 2003, “Representations of Disability and the Personal Relationships of Women with Disabilities”, in Banks and Kaschak 2003: 127–44.
- Davis, Lennard J., 2002, Bending over Backwards: Disability, Dismodernism & Other Difficult Positions , New York: New York University Press.
- Davis, N. Ann, 2005, “Invisible Disability”, Ethics , 116(1): 153–213. doi:10.1086/453151
- Edwards, Steven D., 1997, “Dismantling the Disability/Handicap Distinction”, Journal of Medicine and Philosophy , 22(6): 589–606. doi:10.1093/jmp/22.6.589
- Francis, Leslie, 2018, “Understanding Disability Civil Rights Non-Categorically: The Minority Body and the Americans with Disabilities Act”, Philosophical Studies , 175(5): 1135–1149. doi:10.1007/s11098-018-1067-x
- Garland-Thomson, Rosemarie, 2012, “The Case for Conserving Disability”, Journal of Bioethical Inquiry , 9(3): 339–355. doi:10.1007/s11673-012-9380-0
- Gill, C. J., 2000, “Health Professionals, Disability, and Assisted Suicide: An Examination of Relevant Empirical Evidence and Reply to Batavia”, Psychology, Public Policy, and Law: An Official Law Review of the University of Arizona College of Law and the University of Miami School of Law , 6(2): 526–545.
- Gliedman, John and William Roth, 1980, The Unexpected Minority: Handicapped Children in America , New York: Harcourt Brace Jovanovich.
- Goering, Sara, 2008, “‘You Say You’re Happy, But…’: Contested Quality of Life Judgments in Bioethics and Disability Studies”, Journal of Bioethical Inquiry , 5(2–3): 125–135. doi:10.1007/s11673-007-9076-z
- Goffman, Erving, 1963, Stigma: Notes on the Maintenance of Spoiled Identity , Englewood Cliffs, NJ: Prentiss Hall.
- Gregory, Alex, 2020, “Disability as Inability”, Journal of Ethics and Social Philosophy , 18(1): 23–48. doi:10.26556/jesp.v18i1.572
- Hacking, Ian, 1990, “The Normal State”, in The Taming of Chance , Cambridge: Cambridge University Press, pp. 161–169.
- Hahn, Harlan, 1987 [1997], “Advertising the Acceptably Employable Image: Disability and Capitalism”, Policy Studies Journal , 15(3): 551–570. Reprinted in The Disability Studies Reader , L. J. Davis (ed.), London, UK: Routledge Kegan Paul, 1997, pp. 172–186. doi:10.1111/j.1541-0072.1987.tb00729.x
- Haslanger, Sally, 2000, “Gender and Race: (What) Are They? (What) Do We Want Them To Be?”, Noûs , 34(1): 31–55. doi:10.1111/0029-4624.00201
- Howard, Dana and Sean Aas, 2018, “On Valuing Impairment”, Philosophical Studies , 175(5): 1113. doi:10.1007/s11098-018-1074-y
- Jenkins, Katharine and Aness Kim Webster, 2021, “Disability, Impairment, and Marginalised Functioning”, Australasian Journal of Philosophy , 99(4): 730–747. doi:10.1080/00048402.2020.1799048
- Johnson, Mary, 2003, Make Them Go Away: Clint Eastwood, Christopher Reeve and the Case Against Disability Rights , Louisville, KY: Advocado Press.
- Kahane, Guy and Julian Savulescu, 2009, “The Welfarist Account of Disability”, in Disability and Disadvantage , Kimberley Brownlee and Adam Cureton (eds.), New York: Oxford University Press, pp. 14–53. doi:10.1093/acprof:osobl/9780199234509.003.0002
- Kingma, Elselijn, 2007, “What Is It to Be Healthy?”, Analysis , 67(2): 128–133. doi:10.1093/analys/67.2.128
- Lim, Chong-Ming, 2018, “Disabilities Are Also Legitimately Medically Interesting Constraints on Legitimate Interests”, Mind , 127(508): 977–1002. doi:10.1093/mind/fzy028
- Magee, Bryan and Martin Milligan, 1995, On Blindness: Letters between Bryan Magee and Martin Milligan , New York: Oxford University Press.
- Martiny, Kristian Moltke, 2015, “How to Develop a Phenomenological Model of Disability”, Medicine, Health Care and Philosophy , 18(4): 553–565. doi:10.1007/s11019-015-9625-x
- Menzel, P. T., 1992, “Oregon’s Denial: Disabilities and Quality of Life”, Hastings Center Report , 22(6): 21–25.
- Nordenfelt, Lennart, 1997, “The Importance of a Disability/Handicap Distinction”, Journal of Medicine and Philosophy , 22(6): 607–622. doi:10.1093/jmp/22.6.607
- Oliver, Michael, 1990, The Politics of Disablement , Basingstoke, UK: Macmillan
- Putnam, Ruth Anna, 1995, “Why Not a Feminist Theory of Justice?” in Women, Culture and Development: A Study of Human Capabilities , Martha Nussbaum and Jonathan Glover (eds.), Oxford: Clarendon Press, pp. 298–331.
- Safilios-Rothschild, Constantina, 1970, The Sociology and Social Psychology of Disability and Rehabilitation , New York: Random House.
- Samaha, Adam M. 2007, “What Good Is the Social Model of Disability?,” University of Chicago Law Review : 22(4), 1251–1308. doi:10.2307/20141862
- Savulescu, Julian and Guy Kahane, 2011, “Disability: A Welfarist Approach”, Clinical Ethics , 6(1): 45–51. doi:10.1258/ce.2011.011010
- Schneider, Joseph W., and Peter Conrad, 1985, Having Epilepsy: The Experience and Control of Illness , Philadelphia, PA: Temple University Press.
- Scotch, Richard K. and Kay Schriner, 1997, “Disability as Human Variation: Implications for Policy”, The ANNALS of the American Academy of Political and Social Science , 549(1): 148–159. doi:10.1177/0002716297549001011
- Sen, Amartya, 1993, “Capability and Well‐Being”, in The Quality of Life , Martha Nussbaum and Amartya Sen (eds.), Oxford: Clarendon Press, pp. 30–53. doi:10.1093/0198287976.003.0003
- Shakespeare, Tom, 2006, Disability Rights and Wrongs , London: Routledge.
- Shakespeare, Tom, Kath Gillespie-Sells, and Dominic Davies, 1996, The Sexual Politics of Disability: Untold Desires , London, UK: Cassell.
- Silvers, Anita, 2003, “On the Possibility and Desirability of Constructing a Neutral Conception of Disability”, Theoretical Medicine and Bioethics , 24(6): 471–487. doi:10.1023/B:META.0000006924.82156.5b
- Stone, Karen G., 1997, Awakening to Disability: Nothing About Us Without Us , Volcano, CA: Volcano Press.
- Swain, John and Sally French, 2000, “Towards an Affirmation Model of Disability”, Disability & Society , 15(4): 569–582. doi:10.1080/09687590050058189
- Terzi, Lorella, 2004, “The Social Model of Disability: A Philosophical Critique”, Journal of Applied Philosophy , 21(2): 141–157. doi:10.1111/j.0264-3758.2004.00269.x
- –––, 2009, “Vagaries of the Natural Lottery? Human Diversity, Disability, and Justice”, in Disability and Disadvantage , Kimberley Brownlee and Adam Cureton (eds.), New York: Oxford University Press, pp. 86–111. doi:10.1093/acprof:osobl/9780199234509.003.0004
- Tremain, Shelley, 2001, “On the Government of Disability”, Social Theory and Practice , 27(4): 617–636. doi:10.5840/soctheorpract200127432
- –––, 2017, Foucault and Feminist Philosophy of Disability, Ann Arbor, MI: Michigan University Press.
- UPIAS, 1976, Fundamental Principles of Disability , London: Union of the Physically Impaired Against Segregation.
- Wakefield, Jerome C., 1992, “The Concept of Mental Disorder: On the Boundary between Biological Facts and Social Values”, American Psychologist , 47(3): 373–388. doi:10.1037/0003-066X.47.3.373
- Wasserman, David, 2001, “Philosophical Issues in the Definition and Social Response to Disability”, in Albrecht, Seelman, and Bury 2001: 219–251.
- –––, 2018, “The Minority Body: A Theory of Disability”, The Philosophical Review , 127(2): 251–256. doi:10.1215/00318108-4326667
- Wates, Michael, 1997, Disabled Parents: Dispelling of the Myths , Cambridge, UK: National Childbirth Trust Publishing.
- World Health Organization, 1980, International Classification of Impairment, Disability and Handicap (ICIDH), Geneva: World Health Organization.
- –––, 2001 [ICF], International Classification of Functioning, Disability and Health , Geneva: World Health Organization. [ WHO 2001 available online .]
- Wright, Beatrice A., 1983, Physical Disability: A Psychosocial Approach , second edition, New York: Harper & Row.
- Zola, Irving Kenneth, 1989, “Toward the Necessary Universalizing of a Disability Policy”, The Milbank Quarterly , 67(S3): 401–428.
How to cite this entry . Preview the PDF version of this entry at the Friends of the SEP Society . Look up topics and thinkers related to this entry at the Internet Philosophy Ontology Project (InPhO). Enhanced bibliography for this entry at PhilPapers , with links to its database.
- [ADA] [ Americans with Disabilities Act of 1990, As Amended
- American Philosophical Association Studies (formerly Newsletters) , These includes (among others) studies/newsletters on: Philosophy and the Black Experience; Feminism and Philosophy; Philosophy and Lesbian, Gay, Bisexual, and Transgender Issues; Hispanic/Latino Issues in Philosophy.
- Disability Discrimination Act 1995 , United Kingdom
- International Classification of Functioning, Disability and Health , World Health Organization web page.
[Please contact the author with other suggestions.]
disability: and health care rationing | disability: and justice | disability: health, well-being, personal relationships | feminist philosophy, topics: perspectives on disability | feminist philosophy, topics: perspectives on sex and gender | health | knowledge: analysis of | Molyneux’s problem | self-knowledge
Copyright © 2022 by David Wasserman < dtwasserm @ gmail . com > Sean Aas < sda46 @ georgetown . edu >
- Accessibility
Support SEP
Mirror sites.
View this site from another server:
- Info about mirror sites
The Stanford Encyclopedia of Philosophy is copyright © 2024 by The Metaphysics Research Lab , Department of Philosophy, Stanford University
Library of Congress Catalog Data: ISSN 1095-5054
- Search Menu
- Browse content in Arts and Humanities
- Browse content in Archaeology
- Anglo-Saxon and Medieval Archaeology
- Archaeological Methodology and Techniques
- Archaeology by Region
- Archaeology of Religion
- Archaeology of Trade and Exchange
- Biblical Archaeology
- Contemporary and Public Archaeology
- Environmental Archaeology
- Historical Archaeology
- History and Theory of Archaeology
- Industrial Archaeology
- Landscape Archaeology
- Mortuary Archaeology
- Prehistoric Archaeology
- Underwater Archaeology
- Urban Archaeology
- Zooarchaeology
- Browse content in Architecture
- Architectural Structure and Design
- History of Architecture
- Residential and Domestic Buildings
- Theory of Architecture
- Browse content in Art
- Art Subjects and Themes
- History of Art
- Industrial and Commercial Art
- Theory of Art
- Biographical Studies
- Byzantine Studies
- Browse content in Classical Studies
- Classical Literature
- Classical Reception
- Classical History
- Classical Philosophy
- Classical Mythology
- Classical Art and Architecture
- Classical Oratory and Rhetoric
- Greek and Roman Papyrology
- Greek and Roman Archaeology
- Greek and Roman Epigraphy
- Greek and Roman Law
- Late Antiquity
- Religion in the Ancient World
- Digital Humanities
- Browse content in History
- Colonialism and Imperialism
- Diplomatic History
- Environmental History
- Genealogy, Heraldry, Names, and Honours
- Genocide and Ethnic Cleansing
- Historical Geography
- History by Period
- History of Emotions
- History of Agriculture
- History of Education
- History of Gender and Sexuality
- Industrial History
- Intellectual History
- International History
- Labour History
- Legal and Constitutional History
- Local and Family History
- Maritime History
- Military History
- National Liberation and Post-Colonialism
- Oral History
- Political History
- Public History
- Regional and National History
- Revolutions and Rebellions
- Slavery and Abolition of Slavery
- Social and Cultural History
- Theory, Methods, and Historiography
- Urban History
- World History
- Browse content in Language Teaching and Learning
- Language Learning (Specific Skills)
- Language Teaching Theory and Methods
- Browse content in Linguistics
- Applied Linguistics
- Cognitive Linguistics
- Computational Linguistics
- Forensic Linguistics
- Grammar, Syntax and Morphology
- Historical and Diachronic Linguistics
- History of English
- Language Evolution
- Language Reference
- Language Variation
- Language Families
- Language Acquisition
- Lexicography
- Linguistic Anthropology
- Linguistic Theories
- Linguistic Typology
- Phonetics and Phonology
- Psycholinguistics
- Sociolinguistics
- Translation and Interpretation
- Writing Systems
- Browse content in Literature
- Bibliography
- Children's Literature Studies
- Literary Studies (Romanticism)
- Literary Studies (American)
- Literary Studies (Modernism)
- Literary Studies (Asian)
- Literary Studies (European)
- Literary Studies (Eco-criticism)
- Literary Studies - World
- Literary Studies (1500 to 1800)
- Literary Studies (19th Century)
- Literary Studies (20th Century onwards)
- Literary Studies (African American Literature)
- Literary Studies (British and Irish)
- Literary Studies (Early and Medieval)
- Literary Studies (Fiction, Novelists, and Prose Writers)
- Literary Studies (Gender Studies)
- Literary Studies (Graphic Novels)
- Literary Studies (History of the Book)
- Literary Studies (Plays and Playwrights)
- Literary Studies (Poetry and Poets)
- Literary Studies (Postcolonial Literature)
- Literary Studies (Queer Studies)
- Literary Studies (Science Fiction)
- Literary Studies (Travel Literature)
- Literary Studies (War Literature)
- Literary Studies (Women's Writing)
- Literary Theory and Cultural Studies
- Mythology and Folklore
- Shakespeare Studies and Criticism
- Browse content in Media Studies
- Browse content in Music
- Applied Music
- Dance and Music
- Ethics in Music
- Ethnomusicology
- Gender and Sexuality in Music
- Medicine and Music
- Music Cultures
- Music and Media
- Music and Culture
- Music and Religion
- Music Education and Pedagogy
- Music Theory and Analysis
- Musical Scores, Lyrics, and Libretti
- Musical Structures, Styles, and Techniques
- Musicology and Music History
- Performance Practice and Studies
- Race and Ethnicity in Music
- Sound Studies
- Browse content in Performing Arts
- Browse content in Philosophy
- Aesthetics and Philosophy of Art
- Epistemology
- Feminist Philosophy
- History of Western Philosophy
- Metaphysics
- Moral Philosophy
- Non-Western Philosophy
- Philosophy of Language
- Philosophy of Mind
- Philosophy of Perception
- Philosophy of Action
- Philosophy of Law
- Philosophy of Religion
- Philosophy of Science
- Philosophy of Mathematics and Logic
- Practical Ethics
- Social and Political Philosophy
- Browse content in Religion
- Biblical Studies
- Christianity
- East Asian Religions
- History of Religion
- Judaism and Jewish Studies
- Qumran Studies
- Religion and Education
- Religion and Health
- Religion and Politics
- Religion and Science
- Religion and Law
- Religion and Art, Literature, and Music
- Religious Studies
- Browse content in Society and Culture
- Cookery, Food, and Drink
- Cultural Studies
- Customs and Traditions
- Ethical Issues and Debates
- Hobbies, Games, Arts and Crafts
- Lifestyle, Home, and Garden
- Natural world, Country Life, and Pets
- Popular Beliefs and Controversial Knowledge
- Sports and Outdoor Recreation
- Technology and Society
- Travel and Holiday
- Visual Culture
- Browse content in Law
- Arbitration
- Browse content in Company and Commercial Law
- Commercial Law
- Company Law
- Browse content in Comparative Law
- Systems of Law
- Competition Law
- Browse content in Constitutional and Administrative Law
- Government Powers
- Judicial Review
- Local Government Law
- Military and Defence Law
- Parliamentary and Legislative Practice
- Construction Law
- Contract Law
- Browse content in Criminal Law
- Criminal Procedure
- Criminal Evidence Law
- Sentencing and Punishment
- Employment and Labour Law
- Environment and Energy Law
- Browse content in Financial Law
- Banking Law
- Insolvency Law
- History of Law
- Human Rights and Immigration
- Intellectual Property Law
- Browse content in International Law
- Private International Law and Conflict of Laws
- Public International Law
- IT and Communications Law
- Jurisprudence and Philosophy of Law
- Law and Society
- Law and Politics
- Browse content in Legal System and Practice
- Courts and Procedure
- Legal Skills and Practice
- Primary Sources of Law
- Regulation of Legal Profession
- Medical and Healthcare Law
- Browse content in Policing
- Criminal Investigation and Detection
- Police and Security Services
- Police Procedure and Law
- Police Regional Planning
- Browse content in Property Law
- Personal Property Law
- Study and Revision
- Terrorism and National Security Law
- Browse content in Trusts Law
- Wills and Probate or Succession
- Browse content in Medicine and Health
- Browse content in Allied Health Professions
- Arts Therapies
- Clinical Science
- Dietetics and Nutrition
- Occupational Therapy
- Operating Department Practice
- Physiotherapy
- Radiography
- Speech and Language Therapy
- Browse content in Anaesthetics
- General Anaesthesia
- Neuroanaesthesia
- Clinical Neuroscience
- Browse content in Clinical Medicine
- Acute Medicine
- Cardiovascular Medicine
- Clinical Genetics
- Clinical Pharmacology and Therapeutics
- Dermatology
- Endocrinology and Diabetes
- Gastroenterology
- Genito-urinary Medicine
- Geriatric Medicine
- Infectious Diseases
- Medical Toxicology
- Medical Oncology
- Pain Medicine
- Palliative Medicine
- Rehabilitation Medicine
- Respiratory Medicine and Pulmonology
- Rheumatology
- Sleep Medicine
- Sports and Exercise Medicine
- Community Medical Services
- Critical Care
- Emergency Medicine
- Forensic Medicine
- Haematology
- History of Medicine
- Browse content in Medical Skills
- Clinical Skills
- Communication Skills
- Nursing Skills
- Surgical Skills
- Medical Ethics
- Browse content in Medical Dentistry
- Oral and Maxillofacial Surgery
- Paediatric Dentistry
- Restorative Dentistry and Orthodontics
- Surgical Dentistry
- Medical Statistics and Methodology
- Browse content in Neurology
- Clinical Neurophysiology
- Neuropathology
- Nursing Studies
- Browse content in Obstetrics and Gynaecology
- Gynaecology
- Occupational Medicine
- Ophthalmology
- Otolaryngology (ENT)
- Browse content in Paediatrics
- Neonatology
- Browse content in Pathology
- Chemical Pathology
- Clinical Cytogenetics and Molecular Genetics
- Histopathology
- Medical Microbiology and Virology
- Patient Education and Information
- Browse content in Pharmacology
- Psychopharmacology
- Browse content in Popular Health
- Caring for Others
- Complementary and Alternative Medicine
- Self-help and Personal Development
- Browse content in Preclinical Medicine
- Cell Biology
- Molecular Biology and Genetics
- Reproduction, Growth and Development
- Primary Care
- Professional Development in Medicine
- Browse content in Psychiatry
- Addiction Medicine
- Child and Adolescent Psychiatry
- Forensic Psychiatry
- Learning Disabilities
- Old Age Psychiatry
- Psychotherapy
- Browse content in Public Health and Epidemiology
- Epidemiology
- Public Health
- Browse content in Radiology
- Clinical Radiology
- Interventional Radiology
- Nuclear Medicine
- Radiation Oncology
- Reproductive Medicine
- Browse content in Surgery
- Cardiothoracic Surgery
- Gastro-intestinal and Colorectal Surgery
- General Surgery
- Neurosurgery
- Paediatric Surgery
- Peri-operative Care
- Plastic and Reconstructive Surgery
- Surgical Oncology
- Transplant Surgery
- Trauma and Orthopaedic Surgery
- Vascular Surgery
- Browse content in Science and Mathematics
- Browse content in Biological Sciences
- Aquatic Biology
- Biochemistry
- Bioinformatics and Computational Biology
- Developmental Biology
- Ecology and Conservation
- Evolutionary Biology
- Genetics and Genomics
- Microbiology
- Molecular and Cell Biology
- Natural History
- Plant Sciences and Forestry
- Research Methods in Life Sciences
- Structural Biology
- Systems Biology
- Zoology and Animal Sciences
- Browse content in Chemistry
- Analytical Chemistry
- Computational Chemistry
- Crystallography
- Environmental Chemistry
- Industrial Chemistry
- Inorganic Chemistry
- Materials Chemistry
- Medicinal Chemistry
- Mineralogy and Gems
- Organic Chemistry
- Physical Chemistry
- Polymer Chemistry
- Study and Communication Skills in Chemistry
- Theoretical Chemistry
- Browse content in Computer Science
- Artificial Intelligence
- Computer Architecture and Logic Design
- Game Studies
- Human-Computer Interaction
- Mathematical Theory of Computation
- Programming Languages
- Software Engineering
- Systems Analysis and Design
- Virtual Reality
- Browse content in Computing
- Business Applications
- Computer Games
- Computer Security
- Computer Networking and Communications
- Digital Lifestyle
- Graphical and Digital Media Applications
- Operating Systems
- Browse content in Earth Sciences and Geography
- Atmospheric Sciences
- Environmental Geography
- Geology and the Lithosphere
- Maps and Map-making
- Meteorology and Climatology
- Oceanography and Hydrology
- Palaeontology
- Physical Geography and Topography
- Regional Geography
- Soil Science
- Urban Geography
- Browse content in Engineering and Technology
- Agriculture and Farming
- Biological Engineering
- Civil Engineering, Surveying, and Building
- Electronics and Communications Engineering
- Energy Technology
- Engineering (General)
- Environmental Science, Engineering, and Technology
- History of Engineering and Technology
- Mechanical Engineering and Materials
- Technology of Industrial Chemistry
- Transport Technology and Trades
- Browse content in Environmental Science
- Applied Ecology (Environmental Science)
- Conservation of the Environment (Environmental Science)
- Environmental Sustainability
- Environmentalist Thought and Ideology (Environmental Science)
- Management of Land and Natural Resources (Environmental Science)
- Natural Disasters (Environmental Science)
- Nuclear Issues (Environmental Science)
- Pollution and Threats to the Environment (Environmental Science)
- Social Impact of Environmental Issues (Environmental Science)
- History of Science and Technology
- Browse content in Materials Science
- Ceramics and Glasses
- Composite Materials
- Metals, Alloying, and Corrosion
- Nanotechnology
- Browse content in Mathematics
- Applied Mathematics
- Biomathematics and Statistics
- History of Mathematics
- Mathematical Education
- Mathematical Finance
- Mathematical Analysis
- Numerical and Computational Mathematics
- Probability and Statistics
- Pure Mathematics
- Browse content in Neuroscience
- Cognition and Behavioural Neuroscience
- Development of the Nervous System
- Disorders of the Nervous System
- History of Neuroscience
- Invertebrate Neurobiology
- Molecular and Cellular Systems
- Neuroendocrinology and Autonomic Nervous System
- Neuroscientific Techniques
- Sensory and Motor Systems
- Browse content in Physics
- Astronomy and Astrophysics
- Atomic, Molecular, and Optical Physics
- Biological and Medical Physics
- Classical Mechanics
- Computational Physics
- Condensed Matter Physics
- Electromagnetism, Optics, and Acoustics
- History of Physics
- Mathematical and Statistical Physics
- Measurement Science
- Nuclear Physics
- Particles and Fields
- Plasma Physics
- Quantum Physics
- Relativity and Gravitation
- Semiconductor and Mesoscopic Physics
- Browse content in Psychology
- Affective Sciences
- Clinical Psychology
- Cognitive Psychology
- Cognitive Neuroscience
- Criminal and Forensic Psychology
- Developmental Psychology
- Educational Psychology
- Evolutionary Psychology
- Health Psychology
- History and Systems in Psychology
- Music Psychology
- Neuropsychology
- Organizational Psychology
- Psychological Assessment and Testing
- Psychology of Human-Technology Interaction
- Psychology Professional Development and Training
- Research Methods in Psychology
- Social Psychology
- Browse content in Social Sciences
- Browse content in Anthropology
- Anthropology of Religion
- Human Evolution
- Medical Anthropology
- Physical Anthropology
- Regional Anthropology
- Social and Cultural Anthropology
- Theory and Practice of Anthropology
- Browse content in Business and Management
- Business Ethics
- Business History
- Business Strategy
- Business and Technology
- Business and Government
- Business and the Environment
- Comparative Management
- Corporate Governance
- Corporate Social Responsibility
- Entrepreneurship
- Health Management
- Human Resource Management
- Industrial and Employment Relations
- Industry Studies
- Information and Communication Technologies
- International Business
- Knowledge Management
- Management and Management Techniques
- Operations Management
- Organizational Theory and Behaviour
- Pensions and Pension Management
- Public and Nonprofit Management
- Strategic Management
- Supply Chain Management
- Browse content in Criminology and Criminal Justice
- Criminal Justice
- Criminology
- Forms of Crime
- International and Comparative Criminology
- Youth Violence and Juvenile Justice
- Development Studies
- Browse content in Economics
- Agricultural, Environmental, and Natural Resource Economics
- Asian Economics
- Behavioural Finance
- Behavioural Economics and Neuroeconomics
- Econometrics and Mathematical Economics
- Economic History
- Economic Methodology
- Economic Systems
- Economic Development and Growth
- Financial Markets
- Financial Institutions and Services
- General Economics and Teaching
- Health, Education, and Welfare
- History of Economic Thought
- International Economics
- Labour and Demographic Economics
- Law and Economics
- Macroeconomics and Monetary Economics
- Microeconomics
- Public Economics
- Urban, Rural, and Regional Economics
- Welfare Economics
- Browse content in Education
- Adult Education and Continuous Learning
- Care and Counselling of Students
- Early Childhood and Elementary Education
- Educational Equipment and Technology
- Educational Strategies and Policy
- Higher and Further Education
- Organization and Management of Education
- Philosophy and Theory of Education
- Schools Studies
- Secondary Education
- Teaching of a Specific Subject
- Teaching of Specific Groups and Special Educational Needs
- Teaching Skills and Techniques
- Browse content in Environment
- Applied Ecology (Social Science)
- Climate Change
- Conservation of the Environment (Social Science)
- Environmentalist Thought and Ideology (Social Science)
- Natural Disasters (Environment)
- Social Impact of Environmental Issues (Social Science)
- Browse content in Human Geography
- Cultural Geography
- Economic Geography
- Political Geography
- Browse content in Interdisciplinary Studies
- Communication Studies
- Museums, Libraries, and Information Sciences
- Browse content in Politics
- African Politics
- Asian Politics
- Chinese Politics
- Comparative Politics
- Conflict Politics
- Elections and Electoral Studies
- Environmental Politics
- European Union
- Foreign Policy
- Gender and Politics
- Human Rights and Politics
- Indian Politics
- International Relations
- International Organization (Politics)
- International Political Economy
- Irish Politics
- Latin American Politics
- Middle Eastern Politics
- Political Behaviour
- Political Economy
- Political Institutions
- Political Theory
- Political Methodology
- Political Communication
- Political Philosophy
- Political Sociology
- Politics and Law
- Public Policy
- Public Administration
- Quantitative Political Methodology
- Regional Political Studies
- Russian Politics
- Security Studies
- State and Local Government
- UK Politics
- US Politics
- Browse content in Regional and Area Studies
- African Studies
- Asian Studies
- East Asian Studies
- Japanese Studies
- Latin American Studies
- Middle Eastern Studies
- Native American Studies
- Scottish Studies
- Browse content in Research and Information
- Research Methods
- Browse content in Social Work
- Addictions and Substance Misuse
- Adoption and Fostering
- Care of the Elderly
- Child and Adolescent Social Work
- Couple and Family Social Work
- Developmental and Physical Disabilities Social Work
- Direct Practice and Clinical Social Work
- Emergency Services
- Human Behaviour and the Social Environment
- International and Global Issues in Social Work
- Mental and Behavioural Health
- Social Justice and Human Rights
- Social Policy and Advocacy
- Social Work and Crime and Justice
- Social Work Macro Practice
- Social Work Practice Settings
- Social Work Research and Evidence-based Practice
- Welfare and Benefit Systems
- Browse content in Sociology
- Childhood Studies
- Community Development
- Comparative and Historical Sociology
- Economic Sociology
- Gender and Sexuality
- Gerontology and Ageing
- Health, Illness, and Medicine
- Marriage and the Family
- Migration Studies
- Occupations, Professions, and Work
- Organizations
- Population and Demography
- Race and Ethnicity
- Social Theory
- Social Movements and Social Change
- Social Research and Statistics
- Social Stratification, Inequality, and Mobility
- Sociology of Religion
- Sociology of Education
- Sport and Leisure
- Urban and Rural Studies
- Browse content in Warfare and Defence
- Defence Strategy, Planning, and Research
- Land Forces and Warfare
- Military Administration
- Military Life and Institutions
- Naval Forces and Warfare
- Other Warfare and Defence Issues
- Peace Studies and Conflict Resolution
- Weapons and Equipment

- < Previous chapter
- Next chapter >
2 Models of Disability
- Published: October 2017
- Cite Icon Cite
- Permissions Icon Permissions
The purpose of this chapter is to describe the different models of disability to help sport and exercise psychology researchers understand the various philosophical and psychological perspectives embedded in each model. First examined is the medical model and how it frames disability as a personal flaw and a medical condition that needs fixing. The social model follows, which suggests that while people might have an impairment it is the physical and social environment that causes disability. The third model discussed is the social-relational model, which acknowledges that people’s physical impairment, the built environment, and other people’s attitudes can all influence the experience of disability. In the tragedy model, people have the cultural viewpoint that having an impairment is tragic, that people with disabilities have a poor quality of life and should be pitied. Finally, the affirmation model repudiates the tragedy model and suggests that having a disability, while challenging, is often embraced and can result in benefits. The strengths and weaknesses of all models are discussed and examples of disability sport psychology research are used to illustrate the models.
Signed in as
Institutional accounts.
- Google Scholar Indexing
- GoogleCrawler [DO NOT DELETE]
Personal account
- Sign in with email/username & password
- Get email alerts
- Save searches
- Purchase content
- Activate your purchase/trial code
Institutional access
- Sign in with a library card Sign in with username/password Recommend to your librarian
- Institutional account management
- Get help with access
Access to content on Oxford Academic is often provided through institutional subscriptions and purchases. If you are a member of an institution with an active account, you may be able to access content in one of the following ways:
IP based access
Typically, access is provided across an institutional network to a range of IP addresses. This authentication occurs automatically, and it is not possible to sign out of an IP authenticated account.
Sign in through your institution
Choose this option to get remote access when outside your institution. Shibboleth/Open Athens technology is used to provide single sign-on between your institution’s website and Oxford Academic.
- Click Sign in through your institution.
- Select your institution from the list provided, which will take you to your institution's website to sign in.
- When on the institution site, please use the credentials provided by your institution. Do not use an Oxford Academic personal account.
- Following successful sign in, you will be returned to Oxford Academic.
If your institution is not listed or you cannot sign in to your institution’s website, please contact your librarian or administrator.
Sign in with a library card
Enter your library card number to sign in. If you cannot sign in, please contact your librarian.
Society Members
Society member access to a journal is achieved in one of the following ways:
Sign in through society site
Many societies offer single sign-on between the society website and Oxford Academic. If you see ‘Sign in through society site’ in the sign in pane within a journal:
- Click Sign in through society site.
- When on the society site, please use the credentials provided by that society. Do not use an Oxford Academic personal account.
If you do not have a society account or have forgotten your username or password, please contact your society.
Sign in using a personal account
Some societies use Oxford Academic personal accounts to provide access to their members. See below.
A personal account can be used to get email alerts, save searches, purchase content, and activate subscriptions.
Some societies use Oxford Academic personal accounts to provide access to their members.
Viewing your signed in accounts
Click the account icon in the top right to:
- View your signed in personal account and access account management features.
- View the institutional accounts that are providing access.
Signed in but can't access content
Oxford Academic is home to a wide variety of products. The institutional subscription may not cover the content that you are trying to access. If you believe you should have access to that content, please contact your librarian.
For librarians and administrators, your personal account also provides access to institutional account management. Here you will find options to view and activate subscriptions, manage institutional settings and access options, access usage statistics, and more.
Our books are available by subscription or purchase to libraries and institutions.
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Rights and permissions
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
NC Accessibility Hub
What are you looking for, disability: perspectives and models.
Review different perspectives and concepts of disability as well as models of disability.
Reading Time

Share this article
Introduction.
How disability is constructed and perceived ultimately determines and influences how larger societal systems treat disabled individuals. Moving past definitions and models of disability that focus on negative embodiments, inability, and deficiency is critical if we are to consider accessibility and equity for disabled individuals in our teaching and learning institutions.
Below, we review some of the key framings of disability as well as the medical and social models of disability. When approaching these topics, it is important to consider the implications that certain framings of disability have within larger society.
Disability is not a static term and there is not a ‘one size fits all’ catch all definition that will capture precisely what disability means and is for one person. Disability is a diverse and unique experience — how one person experiences disability will be different from the next. A variety of definitions and perspectives of disability exist that reflect the diverse contexts that they were developed within including bureaucratic institutions, systems of discrimination, advocacy and resistance movements, social and disability justice realms, and more.
Disability is often construed as something that is ‘not normal’ while individuals who are considered ‘able’ are taken for granted as being ‘normal.’ The very classification of ability and normalcy contributes to marginalization:
“Disability is a social construction rather than a biological given, and the classification of disability is really a means of normalizing and privileging some bodies while pathologizing, subordinating, and marginalizing others” (Withers, 2012).
The construct of normalcy serves as the basis from which many disabled individuals experience discrimination and a lack of access in a variety of environments. In our ableism/disablism article , we unpack how disability is used as the basis for discrimination and oppression throughout a variety of systems and institutions.
Some definitions of disability are often centered on what a person can and cannot do. As Emily Ladau (2021) reminds us, there are many other ways to define disability that do not reduce it simply to inability and defines disability as “a state of being; a natural part of the human experience.”
There are different kinds of disabilities that exist in countless different ways. Ladau (2021) identifies the following generally recognized broad categories of disabilities:
- Chronic Illnesses can have an ongoing effect on varying aspects of a person’s physical and mental health.
- Communication disorders affect how a person conveys and/or comprehends information.
- Developmental disabilities can affect the trajectory of a person’s physical or cognitive growth.
- Hearing disabilities partially or completely affect a person’s ability to hear.
- Intellectual disabilities can affect a person’s communication, cognition, and personal and interpersonal activities.
- Learning disabilities affect the ways a person can learn, process, and understand different subject areas.
- Mental health disabilities can affect a person’s thoughts, moods, and behavior.
- Neurological disorders can affect different parts of a person’s nervous system, which can in turn affect them in many ways, including physically, cognitively, and emotionally.
- Physical disabilities can affect a person’s movement, dexterity, or stamina.
- Vision disabilities partially or completed affect a person’s ability to see.
(Ladau, 2021, pp. 35-36)
While these categories are helpful for classification, we cannot make assumptions about a person’s disability just from definitions and taxonomies. We cannot make assumptions about how someone’s disability affects them, as disability is an inherently personal experience.
Some disabilities can be temporary (like a broken bone) and some can be acquired. Some disabilities are apparent — meaning that it is “noticeable to other people based on either outward appearance or communication (Ladau, 2021). Conversely, a nonapparent disability “is something you likely can’t tell a person has when looking at or communicating with them” (Ladau, 2021). Apparent and nonapparent disabilities are sometimes referred to as visible and invisible disabilities respectively.
Models of Disability
Different frameworks, or models, of disability exist to “conceptualize disability as it relates to who we are and the world around us” (Ladau, 2021). The Medical and Social Models of Disability are the two most common models of disability, but others exist including the biopsychosocial model, the charity model, the cultural model, the human rights model, and more. Below we review the medical and social models of disability.
The Medical Model
When contextualizing and analyzing disability within larger society, disability studies scholars turn to two models of disability: the medical model and the social model.
The Medical Model of Disability frames disability as the root of the problem that lies with the individual rather than surrounding social structures and systems. Generally, the medical model views disability as a deficiency. The medical model also frames non-disabled individuals and bodies as ‘normal’ and disabled individuals and bodies as ‘abnormal.’ In this model, the disabled individual is essentially the barrier, and it is that person that needs to be addressed in terms of access. The medical model also prioritizes medical diagnoses and documentation as a means of identifying disability as well as receiving accommodations or other services to reduce barriers.
Understandably, the medical model is problematic in many ways. First, the medical model is focused on “fixing the disability to the greatest extent possible” and ‘normalizing’ the individual (Haegele & Hodge, 2016). Second, the medical model posits a normative understanding of disability — disabled people are understood as not being able to function in the ways a ‘normal’ person can (Mitra, 2006). As well, the medical model hyper focuses on the individual while ignoring the systemic issues in society that produce barriers and limit accessibility (deBie & Brown, 2017).
The medical model still dominates much of the services and supports developed to support disabled individuals. For instance, the academic accommodation model is largely based on the medical model of disability with its emphasis on diagnosis and documentation.
The Social Model
The Social Model of Disability was developed as a response to challenges with the medical model. The main idea at the core of the social model is that people are “not disabled by [their] impairments but by the disabling barriers [they] face in society” (Oliver, 2013). There are numerous variants of the social model that generally all posit that the problem is not the person with a disability, but the barriers in the surrounding environment (Mitra, 2006). In the social model of disability, “it is society that imposes disability on individuals with impairments” (Hagele & Hodge, 2016).
The difference between the medical and social models is encapsulated by Brown and Leigh (2018):
“Depending on one’s ontological and epistemological view, disability is either considered as the experience resulting from a biological or medical focus on the personal, or as the experience of social oppression and environmental barriers. Within the binary of the medical versus the social model of disability, impairment or chronic illness focus on the biological and functional, whereas disability reflects the social and environmental response to the biological and functional.”
Some have suggested that the social model is too limited in how it views disability and it fails to take account of the breadth of diverse disability experiences (Oliver, 2013). Critiques of both models exist and “neither the medical nor the social model can exist independently of each other” and no model can fully capture the depth and breadth of disability (Ladau, 2021). Models and frameworks help to inform our understandings of disability and reflect how larger society understands disability. Yet no one model can capture the diversity and complexity of disability writ large.
Summary/Key Takeaways
How disability is constructed, thought of, and perceived influences how disabled staff and students are treated in our teaching and learning institutions. Different models of disability exist to help us conceptualize disability and one’s relationship to surrounding environments. As we think about accessibility and equity for disabled individuals, we must challenge ourselves to deconstruct constructions of ‘normalcy’ and ‘deficiency.’
You might be interested in...

Why Accessibility
Learn why accessibility in postsecondary institutions is critical for disabled students, staff, and faculty.

Ableism/Disablism
Learn what ableism and disablism are and how they operate to discriminate against disabled individuals and communities.
- Photo by SeventyFour via Getty Images. Used with permission.
Brown, N., & Leigh, J. (2018). Ableism in academia: Where are the disabled and ill academics? Disability & Society, 33(6), 985-989.
de Bie, A. & Brown, K. (2017) Forward with flexibility – A teaching and learning resource on accessibility and inclusion. McMaster University: Pressbooks. https://flexforward.pressbooks.com/
Haegele, J. A., & Hodge, S. (2016). Disability discourse: Overview and critiques of the medical and social models. Quest, 68(2), 193-206.
Ladau, E. (2021). Demystifying disability: What to know, what to say, and how to be an ally. California: Ten Speed Press.
Mitra, S. (2006). The capability approach and disability. Journal of Disability Policy Studies, 16, 23-247.
Oliver, M. (2013). The social model of disability: Thirty years on. Disability & Society, 28(7), 1024-1026.
Withers, A.J. (2012). Disability politics & theory. Halifax: Fernwood Publishing.
Is this page useful?
Importance of the Social Model of Disability Essay
People’s perceptions concerning individuals with disabilities determine how they care and live with them in different communities. In this regard, the social model of disability focuses on changing the misconception that people with disabilities have problems, which need medical treatments to be fixed. According to Kattari et al. (2017), the model highlights society’s barriers and blame them for the anguishes experienced by persons with disabilities. Indeed, although they strive to live a prosperous life, external forces rather than medical reasons interrupt their progress and ambitions. For example, it is significant to examine environmental challenges, including buildings, public places, and modes of transport developed without thoughts of people with disabilities’ needs. Therefore, the social model helps individuals visualize the building’s problem for lacking a ramp at the entrance instead of blaming people for their disabilities, which are beyond their control.
Besides, the social model helps eliminate prejudices and stereotypes that prevent disabled individuals from enjoying equal opportunities as other humans in society. For instance, the public perceives people with disabilities as dependents and burdens to their families and communities. Such misunderstandings have inspired negative attitudes, including assuming that a person with a disability cannot work, live independently, and have children (Kattari et al., 2017). The social model helps to change the public conversation and create an environment that guarantees the choice, control, and independence of disabled individuals. In this way, the government and its people can focus on solutions, which eliminate discriminatory conclusions restricting the potential of persons with disabilities. Additionally, the social model encourages the formulation of flexible policies, which incorporate empathy and safeguard all individuals’ rights in society, irrespective of their physical or emotional incapacities. Conclusively, the model suggests solutions that rectify the problems witnessed in the modern and disabling world to remove barriers, which discriminate and isolate people with disabilities.
Kattari, S. K., Lavery, A., & Hasche, L. (2017). Applying a social model of disability across the life span. Journal of Human Behavior in the Social Environment , 27 (8), 865-880. Web.
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2022, February 23). Importance of the Social Model of Disability. https://ivypanda.com/essays/importance-of-the-social-model-of-disability/
"Importance of the Social Model of Disability." IvyPanda , 23 Feb. 2022, ivypanda.com/essays/importance-of-the-social-model-of-disability/.
IvyPanda . (2022) 'Importance of the Social Model of Disability'. 23 February.
IvyPanda . 2022. "Importance of the Social Model of Disability." February 23, 2022. https://ivypanda.com/essays/importance-of-the-social-model-of-disability/.
1. IvyPanda . "Importance of the Social Model of Disability." February 23, 2022. https://ivypanda.com/essays/importance-of-the-social-model-of-disability/.
Bibliography
IvyPanda . "Importance of the Social Model of Disability." February 23, 2022. https://ivypanda.com/essays/importance-of-the-social-model-of-disability/.
- Accidents and Ramp Damage - Aviation
- The Miami International Airport Airline Ramp Workers Strike
- Being Obese as a Disabling Disability: Concerning the Obstacles for Challenged People
- Sports Can Improve the Psychological Well-Being of People with Disability
- Predicting Medium-Term Success Among Alcohol and Opiate Dependents
- The History of Cuban Insurrection: A Feeling of Inequality Among the Citizens and the Need to Rectify This
- The Phenomenon of Victim-Blaming
- Human Cloning Technology and Its Justification
- Child Abuse Versus Elder Abuse
- Safety Management System: Airport Ramps in the UAE
- Social Work as an Important Element of Society
- The Role of a Student in Society
- Changing Attitudes Toward Sickness and the Sick
- Examining Whitfield County
- Unruly Youth in Urban Environments. Analysis
Academia.edu no longer supports Internet Explorer.
To browse Academia.edu and the wider internet faster and more securely, please take a few seconds to upgrade your browser .
Enter the email address you signed up with and we'll email you a reset link.
- We're Hiring!
- Help Center

Models of Disability from Religious Tradition: Introductory Editorial

Journal of Disability & Religion
Related Papers
Deborah Creamer
Disability theology explores the ways in which religious traditions have engaged (or failed to engage) notions of disability and impairment, and offers constructive possibilities for inclusive theological work in the future. This essay reviews four primary models of disability (moral model, medical model, social model, and limits model) and explores how these relate to religious understandings and practices. The image of the Disabled God is highlighted, as are the ways this field has come to engage varieties of disability experience (including cognitive disabilities and autism) and diversity more broadly. Philosophical notions (such as those around normalcy or human flourishing) are explored alongside advocacy and access issues (particularly with regard to religious practices such as preaching, religious education, and biblical interpretation). Future possibilities and directions for disability theology are also proposed.
John Swinton
This research report is less a survey of the literature than a reflection on the emergence, aims and predominant themes to emerge from theological engagements with issues of disability. It advances a rather bold claim: the theology of disability is central to our understanding of what it means to know who God is and to know what it means to be a human being living fully under God. While such a statement will need justification, the emphasis within this essay is that the theology of disability is not a specialist enterprise or those who are “interested in such things.” Theological reflection on human disability leads us into the very heart of the theological enterprise in both its practical and theoretical aspects. As such it has particular significance for practical theology.
HTS Teologiese Studies / Theological Studies
Rantoa Letsosa
Critical reflection on the importance of shaping disability-friendly – or disability-inclusive – congregations has enjoyed increasing attention in the field of practical theology in recent years. Moreover, the development of disability theology is a testament to the fact that practical theologians and the wider church community have taken serious notice of the realities and experiences of people with disabilities in our time. Nevertheless, even before the task of engaging in theological reflection from a disability perspective commences, it is necessary that theologians acquaint themselves with the various models of disability that shape people’s perceptions and ideas about people with disabilities. Guided by the principles of the interpretive task of practical theological investigation and cognizant of the importance of models of disability in shaping perceptions regarding people with disabilities, this article seeks to provide a brief overview of nine of the most dominant models o...
tui nuku Smith
RELATED PAPERS
matias rosales mendez
mariheli jhandira lugo
Mariheli Jhandira Rodriguez Lugo
Surendra Bargali
Nature reviews. Clinical oncology
Kevin Brindle
Rosanna Salvia
Lecture Notes in Computer Science
Rainer Manthey
African Journal of Political Science and International Relations
John Ishiyama
MEDIA ILMU KESEHATAN
lisa novita sari
Revista Brasileira de Buiatria - RBB
Marcelo Molento
VASILIKI KANELLIADOU
Revista chilena de obstetricia y ginecología
Sara Osorio
Proceedings of the IEEE Conference on Decision and Control
sergio bras
Kalam Cendekia: Jurnal Ilmiah Kependidikan
Fitri Nurjayani
selim martin
Atherosclerosis
David Greaves
godwin adahada
American Journal of Epidemiology
Rachael Blair
Putri Anjani
Shelley Craig
Jurnal Intent
resista vikaliana
Mexican Law Review
Gisela Maria Pérez Fuentes
Nawsherwan Sadiq , Ashqi Mohammed
Celine Hudelot
Chinese Business Review
Ryszard Kaminski
hjhjgfg freghrf
RELATED TOPICS
- We're Hiring!
- Help Center
- Find new research papers in:
- Health Sciences
- Earth Sciences
- Cognitive Science
- Mathematics
- Computer Science
- Academia ©2024
COMMENTS
Society's and researchers' conceptualizations of disability have evolved over time. As noted in Enabling America 5 and on the basis of public policy at the time, "In the 1950s, impairment of a given severity was viewed as sufficient to result in disability in all circumstances; in contrast, the absence of impairment of that severity was thought to be sufficient grounds to deny disability ...
In 1965, Saad Z. Nagi published a very influential conceptual model of disablement in which he distinguished among several aspects of the disability phenomenon. In the following decades, several other conceptual models were proposed, increasingly taking up ideas and demands emerging from the disability movement, especially the social model of disability. In this review, three generations of ...
The different models of disability—and particularly, the medical and social models—have always been interpreted as favoring different responses to disability. ... "Introduction: Beyond Pedestals", in Women with Disabilities: Essays in Psychology, Culture, and Politics, Michelle Fine and Adrienne Asch (eds.), Philadelphia, PA: Temple ...
A social model approach. Papers included in the scoping review, regardless of whether they are for or against a social model of disability, were widely seen as foundational to disability studies and advocacy. 198, 306 - 309 A social model of disability developed from the experiences and activism of disabled people in the UK from the early ...
It starts with a brief historical overview of the social model of disability and its relationship to medical sociology. The authors frame their arguments by drawing on empirical research from three separate studies to answer the key question that has dogged disability research and disability studies since its first inception, namely: what are ...
The social model of disability. In response to the traditional medical model of disability, disability activists and scholars have offered a social model of disability [], which relies on a relatively sharp distinction between impairment and disability.Within the social model, impairment is understood as a state of the body that is non-standard, defined as "lacking part of or all of a limb ...
The North American social model of disability is linked to the disability rights movement, developing in tandem with the Civil Rights Movement from the 1960s onwards against racial segregation and discrimination (Frum 2000).Civil rights concepts were then applied to the segregation of disabled people and discrimination against them.
Abstract. In his 2013 article in Disability & Society, Oliver recommended that the social model should either be replaced or re-invigorated.I argue here that the social model's current emphasis reflects the social conditions in which it was introduced, and that the model's impact on disabled people's lives would increase if its emphasis was to more accurately reflect the current social ...
in English This article reviews the status of disability studies, in particular historic disability studies, models of disability to date, and how those models have been used or altered to fit premodern disability studies. It also examines new ideas and models for a broader look at how disabled people are part of larger society, namely Mounsey's model of "Variabilities," Booth's ...
Introduction The objective of this paper is to provide a description and analysis of the social model of disability, and how it has developed during the past 30 years. Both academics working in the field of disability studies, as well as practitioners providing disability services have been increasingly influenced by its underpinning philosophy. Furthermore, the " disability movement ...
An Essay on Modeling: The Social Model of Disability. A. Silvers. Published 2009. Sociology, Philosophy. From its first exposition almost half a century ago, the social model of disability has been aimed at altering both theory and practice, bringing about profound changes in people's understanding of…. Expand.
From a social model perspective, medicine's focus on treating impairment reified the widespread conception of disability as an individual tragedy, rather than the outcome of oppressive social perceptions and arrangements. One way to combat oppression, social model advocates suggested, was to exclude disability from medical oversight.
The term social model of disability was first coined in literature by Oliver (1986) as he interpreted the Foundational Principals of Disability which written by UPIAS in 1967 (see Oliver, 1986 ...
(DOI: 10.1007/978-90-481-2477-0_2) From its first exposition almost half a century ago, the social model of disability has been aimed at altering both theory and practice, bringing about profound changes in people's understanding of disability, and in the daily lives of disabled people as well. The social model's foil, and on some accounts its antithesis, is the medical model of disability ...
One of the most prominent and criticized models of disability is the medical model. The medical model of disability establishes disability as an individual problem (Cameron, 2013, p. 99).Other elements of a medical model include viewing the impairment (e.g., spinal cord injury [SCI]) as disabling instead of society (e.g., a lack of a ramp allowing a wheelchair user to enter a building) as ...
The development of the law in the United Kingdom is predominantly based on disability theories that challenge disability discrimination with reference to mechanisms that label disability as a problem in need of a solution, rather than recognition of disability as different but equal (Goodley et al., 2011).This is in contrast to the more radical models associated with feminism, queer theory and ...
Models of Disability. Different frameworks, or models, of disability exist to "conceptualize disability as it relates to who we are and the world around us" (Ladau, 2021). The Medical and Social Models of Disability are the two most common models of disability, but others exist including the biopsychosocial model, the charity model, the ...
ABSTRACT This article aims to reorient thinking about the relationship between the long-standing social model of disability and the rapidly emerging human rights model. In particular, it contests the influential view that the latter develops and improves upon the former (the improvement thesis) and argues instead that the two models are complementary (the complementarity thesis).
The social model helps to change the public conversation and create an environment that guarantees the choice, control, and independence of disabled individuals. In this way, the government and its people can focus on solutions, which eliminate discriminatory conclusions restricting the potential of persons with disabilities.
Models of Disability and Their Impact on Children's Lives There are two primary models of disability: the medical model and the social model. Medical Model of Disability The. Continue reading. Ask a new question. Discover more from: Introduction to childhood studies and child psychology E102.
Social model is not practised for the autism label. The medical model of disability is the dominant model in autism studies (Graby Citation 2016).The UK full-time employment rate for people with autism is stagnant at around 15% (National Autistic Society Citation 2016).Even with The Autism Act 2009 and The Equality Act 2010, autistic individuals could be discriminated against in the Criminal ...
This essay reviews four primary models of disability (moral model, medical model, social model, and limits model) and explores how these relate to religious understandings and practices. The image of the Disabled God is highlighted, as are the ways this field has come to engage varieties of disability experience (including cognitive ...