- Member Login

Xerostomia (Dry Mouth)
- Severity of xerostomia or dry mouth symptoms ranges from mild oral discomfort to significant oral disease that can compromise the patient’s health, dietary intake, and quality of life.
- Causes of dry mouth can include toxicity from chemotherapy, head and neck radiotherapy, medication intake, autoimmune diseases (e.g., Sjögren disease), or other conditions (e.g., uncontrolled diabetes, infections, hormonal changes).
- Reduced salivary flow can cause difficulties in tasting, chewing, swallowing, and speaking; it can also increase the chance of developing dental caries, demineralization of teeth, tooth sensitivity, and/or oral infections.
- The goals of treating xerostomia include identifying the possible cause(s), relieving discomfort, and preventing complications (e.g., dental caries and periodontal infections).
- Xerostomia may be alleviated by use of saliva substitutes and other interventions (e.g., chewing sugar-free gum). Other oral health-specific recommendations (e.g., brushing teeth gently at least twice a day with fluoridated toothpaste) may help provide relief from or prevent adverse sequelae of dry mouth.
Xerostomia is the subjective sensation of oral dryness. 1, 2 Dry mouth is a common, complex and under-recognized condition, which may or may not be associated with salivary gland hypofunction (i.e., the objective measurement of reduced salivary flow). 3-5
Saliva is a complex mixture of fluids that provides several protective functions, including cleansing the oral cavity, facilitating speech and swallowing, protecting oral tissues (including teeth) against physical and microbial insults, and maintaining a neutral pH. 6 Reduced salivary flow can cause difficulties in tasting, chewing, swallowing, and speaking; it can also increase the chance of developing dental caries, demineralization of teeth, tooth sensitivity, and/or mucosal infections. 4, 7
There are a variety of potential causes of xerostomia, including dehydration, medication use, toxicity of chemotherapy and/or radiation therapy of the head and neck, autoimmune diseases, other chronic diseases, and nerve damage. 8 Patients can be variably affected. 8
Severity of dry mouth symptoms ranges from mild oral discomfort to significant oral disease that can compromise the patient’s health, dietary intake, and quality of life. 1 Estimates of xerostomia prevalence in the general population vary widely depending on case definitions used and differences in study samples (e.g., age range, health status). 9 Previous studies reported xerostomia prevalence estimates ranging from 10 to 26% in men to 10 to 33% in women. 10 A 2018 systematic review reported an overall estimated prevalence of xerostomia in approximately 22% of the global population. 11 Xerostomia prevalence is generally higher among older individuals, typically due to polypharmacy and with the onset of various medical conditions over time. Virtually all patients with Sjögren disease or radiation therapy for head and neck cancer develop dry mouth. 12
Saliva is a mixture of secretions from the major (i.e., parotid, submandibular, sublingual) and minor salivary glands located in the oral mucosa. 13 In healthy individuals, the daily production of saliva normally ranges from 0.5 to 1.5 liters. 14 Saliva is 99% water and less than 1% solids, including a number of electrolytes (e.g., sodium, potassium, calcium, bicarbonate, phosphate) and organic components (e.g., immunoglobulins, proteins, enzymes, mucins). 13, 15 In addition to keeping tissues moist and helping to digest food, saliva cleanses the oral cavity, makes it possible to chew and swallow food, facilitates oral sugar clearance and serves as a buffer that protects oral mucosa against orally ingested acids or regurgitated stomach acid. 1, 7, 16 Salivary proteins and mucins contribute to the lubrication and coating of oral tissues, protecting the mucosa from chemical, microbial, and physical injury (e.g., abrasion). 1, 7 Without adequate salivary flow, tooth decay and a variety of oral infections can develop. 7, 13 Xerostomia symptoms may also worsen at night because salivary output reaches its lowest circadian levels during sleep, and the problem can be exacerbated by mouth breathing. 17
Reduced salivary flow can interfere with chewing or swallowing certain foods which may result in malnutrition. 7 Significant loss of salivary gland function is associated with altered taste sensation (i.e., dysgeusia) 1, 14 and difficulty in swallowing (i.e., dysphagia). 18, 19
Drug/Therapy-Related
Medication-Induced Xerostomia . The most frequent cause of hyposalivation is use of certain medications. 4 A 2018 systematic review concluded that urologic medications, antidepressants and psycholeptics were associated with dry mouth in older adults. 20 Another systematic review (completed in conjunction with the World Workshop of Oral Medicine VI) reported that 106 medications had strong to moderate evidence of being associated with salivary gland dysfunction, including anti-depressants (e.g., fluoxetine) and anti-muscarinic medications (e.g., tolterodine for overactive bladder). 2 An additional 46 medications in the same systematic review 2 were found to have weak evidence of interfering with salivary gland function.
Over-the-counter (OTC) and prescription medications that can contribute to or exacerbate oral dryness include: antihistamines (for allergy or asthma), antihypertensive medications, decongestants, pain medications, diuretics, muscle relaxants, and antidepressants. 8, 13, 21, 22 The most common types of medications causing salivary dysfunction have anticholinergic effects, e.g., tricyclic antidepressants, antihistamines, antihypertensive medications, and antiseizure/antispasmodic drugs. 23 Patients who are taking multiple medications may be at a higher risk of dry mouth as an adverse effect of therapy. 14 Overall, the likelihood of decreased salivary flow rates tends to increase in the presence of numerous diseases and medications; however, individuals may still report and experience the subject sensation of xerostomia while having salivary flow rates that fall within a normal range (i.e., without an observable decrease in salivary flow). 16 Dry mouth is also commonly reported as a minor adverse effect of medical cannabis use, along with drowsiness, dizziness and nausea. 24
Drug substitutions may help reduce the dry mouth effects of certain medications (e.g., selective serotonin-reuptake inhibitor antidepressants tend to cause less dry mouth than tricyclic antidepressants). 17, 23, 25 Dry mouth symptoms from medications may also be reduced if patients who are taking anticholinergic medications can take them during the day, rather than at night (avoiding nocturnal symptoms), and in divided doses, rather than one larger, single dose (potentially avoiding the xerostomic adverse effects). 17, 23
Toxicity Related to Cancer Chemotherapy or Head and Neck Cancer Radiotherapy . Oral complications of cancer chemotherapy or head and neck cancer radiotherapy 13, 23, 26 can be acute (i.e., develop during therapy) or chronic (i.e., develop months to years after therapy). 26 These therapies can cause xerostomia/salivary gland hypofunction via direct toxicity to salivary glands and oral tissues, or indirect damage due to regional or systemic toxicity. 23, 26 Generally, cancer chemotherapy causes acute toxicities that resolve following discontinuation of therapy and healing of damaged tissue, whereas radiation therapy can cause acute oral toxicity, as well as induce permanent tissue damage that can put patients at lifelong risk. 23, 26
Xerostomia can also occur following hematopoietic stem-cell transplantation and as part of salivary gland graft versus host disease. 26 Sialadenitis, or infection of the salivary gland, is another potential acute oral toxicity associated with chemo/radiotherapy. 26 Radioactive iodine, which is used to treat some thyroid cancers, can damage salivary glands (primarily the parotid glands) in a dose-dependent fashion. 17, 23
Physiological or Disease-Related
Aging . Xerostomia affects an estimated 30% of patients older than 65 years and up to 40% of patients older than 80 years; this is primarily an adverse effect of medication(s), although it can also result from comorbid conditions such as diabetes, Alzheimer’s disease, or Parkinson’s disease. 27-29 Xerostomia, while common among older patients, has been found to be twice as likely to occur in adult patients who take one of more drugs daily when compared with medication-free individuals. 30 Xerostomia prevalence is also higher among individuals with an intake of more than four daily prescription medications. 29
Autoimmune Disease . Sjögren disease (formerly known as Sjögren syndrome) is the second most common autoimmune connective-tissue disease, 31 and is the systemic condition most frequently associated with salivary dysfunction and xerostomia. 17 Approximately 90 percent of those with Sjögren disease are women, and patients often experience associated symptoms such as fatigue and joint pain. 32 Although Sjögren disease is a systemic condition that can affect multiple body organs or systems, 33 the primary symptoms are dry mouth and dry eyes. 7, 13, 31 Sjögren disease causes chronic inflammation and dysfunction, and may also result in persistent or recurrent salivary gland swelling. 29, 34, 35
Primary Sjögren disease (i.e., Sjögren disease alone) affects approximately 1 in 70 people; this number approximately doubles if patients with other major autoimmune or rheumatic disease (e.g., rheumatoid arthritis) in addition to Sjögren disease are included 31 (i.e., secondary Sjögren disease 17 ). Other autoimmune diseases that can occur with Sjögren disease include systemic lupus erythematosus, scleroderma, polymyositis, and polyarteritis nodosa. 17
Other Conditions . Other conditions associated with dry mouth include: 1, 7, 8, 13, 21, 36-38
Burning mouth syndrome COVID-19 Cystic fibrosis Graft-versus-host disease Hepatitis C virus infection HIV infection/AIDS Hormonal changes (e.g., pregnancy or menopause) Lymphoma Nerve damage from a head or neck injury Poorly controlled diabetes Psychogenic causes Salivary gland agenesis or aplasia Stroke Uncontrolled hypertension
Potential lifestyle causes of xerostomia include the use of alcohol and tobacco or cannabis use, or the consumption of excessive caffeine or spicy food. 6, 39
- a sticky, dry, or burning feeling in the mouth
- trouble chewing, swallowing, tasting, or speaking
- altered taste or intolerance for spicy, salty, or sour foods or drinks
- a dry or sore throat
- cracked, peeling, atrophic or sticky lips
- a dry, rough tongue
- mouth sores
- oral fungal infection (e.g., candidiasis)
- halitosis (bad breath)
- inability to retain dentures or otherwise poorly fitting removable prostheses
The goals of treating xerostomia include identifying the possible cause(s), relieving discomfort, and preventing complications, e.g., dental caries and periodontal infections. 6
Identification
Patients with complaints of dry mouth should undergo a detailed medical and dental history to help with early detection and identification of potential underlying causes. 1, 17, 29 In patients with xerostomia or salivary gland hypofunction, oral examination may reveal dry and friable oral mucosa and the tongue may appear dry and fissured. 1, 22 Patients may commonly have dental caries (especially root, cervical, or incisal/cuspal tips), plaque accumulation, gingivitis, and/or periodontitis. 1, 22, 40 Infections (e.g., oral candidiasis) and enlargement of salivary glands from sialadenitis may also be present. 1, 17, 22, 40 Other oral manifestations evident on examination may include angular cheilitis, mucositis, traumatic oral lesions, dry lips or dry throat, and/or difficulty in wearing/retaining oral prostheses. 17, 22, 40-42
A thorough extraoral and intraoral examination to identify the presence or absence of salivary pooling on the floor of the mouth can help a dentist identify who will benefit from further diagnostic evaluations, such as salivary flow rate measurement, minor salivary gland biopsy, or blood and microbial tests. 1, 4 Inspection and palpation of major salivary glands may also assist in identifying poor salivary pooling or the presence of masses, swelling or tenderness. 1, 43 A patient is considered to have reduced salivary flow (hyposalivation) if the unstimulated salivary flow is 0.1 mL/min or less (measured for 5 to 15 minutes) or if the chewing-stimulated salivary flow is 0.7 mL/min or less (measured for 5 minutes). 22, 40
General Palliative/Preventive Interventions
Management of xerostomia and hyposalivation should emphasize patient education, adequate hydration and lifestyle modifications. 1, 4 Various palliative and preventive measures, including pharmacologic treatment with salivary stimulants, topical fluoride, saliva substitutes, and use of sugar-free gum/mints, may alleviate some symptoms of dry mouth and may improve a patient’s quality of life. 1, 22
Examples of coping strategies for relieving dry mouth include: 17, 21
- sipping water or sugarless, caffeine-free drinks
- sucking on ice chips
- using lip lubricants frequently (e.g., every two hours)
- chewing sugar-free gum or sucking on sugar-free candy 17
- avoiding salty or spicy food or dry, hard-to-chew foods 17
- avoiding sticky, sugary foods
- avoiding irritants such as alcohol (including alcohol-containing mouthrinses 20 ), tobacco, and caffeine
- drinking fluids while eating carefully 13, 17
- using a humidifier at night 17
Dental and oral health-specific recommendations from the National Institute for Dental and Craniofacial Research 7 and others 17, 22, 23 include the following for patients with dry mouth:
- brush teeth gently at least twice a day with fluoridated toothpaste
- floss teeth every day
- schedule dental visits at least twice a year (with yearly bitewing radiographs)
- use of a prescription-strength fluoride gel (0.4% stannous fluoride, 1.1% sodium fluoride) daily to help prevent dental decay
- prompt treatment of oral fungal or bacterial infections
- application of 0.5% fluoride varnish to teeth
- dental soft- and hard-tissue relines of poorly fitting prostheses and use of denture adhesives
Salivary Stimulants . Salivary stimulants should be considered in patients with residual salivary gland function. 4, 17 Sugar-free chewing gum, candies, and mints can be used to stimulate salivary output. 17 The FDA has approved two oral sialologues--pilocarpine (Salagen ® , Eisai and generics) 44 and cevimeline hydrochloride (Evoxac ® capsules, Daiichi-Sankyo and generics) 45 --to treat dry mouth. 4, 23 Pilocarpine is typically administered at a dose of 5 mg three times a day for at least three months, and cevimeline is prescribed at a dose of 30 mg three times a day for at least three months. 4 Adverse effects include sweating, cutaneous vasodilation, nausea and vomiting, diarrhea, hiccup, hypotension and bradycardia, increased urinary frequency, bronchoconstriction, and vision problems. 4
Artificial Saliva/Saliva Substitutes/Oral Moisturizers . Artificial saliva products and oral moisturizers are available with or without prescription. They typically contain a combination of carboxymethylcellulose and glycerin to increase viscosity, as well as buffering and flavoring agents (e.g., sorbitol, xylitol), and calcium and phosphate ions. 8, 46 Some products also contain fluoride. 8 A prescription-only product, NeutraSal ® (OraPharma, Inc.), is a supersaturated calcium phosphate rinse available as powder for reconstitution. 47
The ADA Seal of Acceptance category for products for temporary relief of dry mouth means that the product is safe and has shown efficacy in temporarily relieving dry mouth symptoms, when used as directed.
Saliva substitutes are used as often as needed and although they do not cure dry mouth, they can provide temporary relief of symptoms. 8 Alcohol-free mouthrinses, lozenges, and moisturizing oral sprays and gels are marketed as OTC oral care options for patients with dry mouth. 8, 13, 17 There are also toothpastes specifically formulated for use in patients with dry mouth. 8, 13
A 2011 Cochrane review 48, 49 found “no strong evidence” that any specific topical therapy (e.g., sprays, lozenges, mouth rinses, gels, oils, chewing gum, or toothpastes) was effective for relieving the symptoms of dry mouth. Although chewing gum was shown to increase saliva production, there was no strong evidence that dry mouth symptoms were improved. The authors noted that “patient preference is an important consideration, together with consideration of the potential adverse effects.” The review concluded that, “Well designed, adequately powered randomized controlled trials of topical interventions for dry mouth, which are designed and reported according to CONSORT guidelines, are required to provide evidence to guide clinical care.” 49
- Plemons JM, Al-Hashimi I, Marek CL, American Dental Association Council on Scientific Affairs. Managing xerostomia and salivary gland hypofunction: executive summary of a report from the American Dental Association Council on Scientific Affairs. J Am Dent Assoc 2014;145(8):867-73.
- Wolff A, Joshi RK, Ekström J, et al. A guide to medications inducing salivary gland dysfunction, xerostomia, and subjective sialorrhea: a systematic review sponsored by the World Workshop on Oral Medicine VI. Drugs R D 2017;17(1):1-28.
- Chaudhury NM, Shirlaw P, Pramanik R, Carpenter GH, Proctor GB. Changes in saliva rheological properties and mucin glycosylation in dry mouth. J Dent Res 2015;94(12):1660-7.
- Villa A, Connell CL, Abati S. Diagnosis and management of xerostomia and hyposalivation. Ther Clin Risk Manag 2015;11:45-51.
- Wiriyakijja P, Niklander S, Santos-Silva AR, et al. World Workshop on Oral Medicine VIII: Development of a core outcome set for dry mouth: a systematic review of outcome domains for xerostomia. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 2023 Mar 6.
- Lynge Pedersen AM, Belstrøm D. The role of natural salivary defences in maintaining a healthy oral microbiota. Journal of Dentistry 2019;80:S3-S12.
- National Institute of Dental and Craniofacial Research. Dry Mouth (NIH Publication No. 14-3174). National Institutes of Health. http://www.nidcr.nih.gov/oralhealth/Topics/DryMouth/DryMouth.htm . Accessed April 20, 2023.
- Terrie YC. Dry mouth: more common and less benign than thought. Pharmacy Times. February 10, 2016. https://www.pharmacytimes.com/view/dry-mouth-more-common-and-less-benign-than-thought Accessed April 20, 2023.
- Ying Joanna ND, Thomson WM. Dry mouth - An overview. Singapore Dent J 2015;36:12-7.
- Furness S, Bryan G, McMillan R, Birchenough S, Worthington HV. Interventions for the management of dry mouth: non-pharmacological interventions. Cochrane Database Syst Rev 2013(9):Cd009603.
- Agostini BA, Cericato GO, Silveira ERD, et al. How Common is Dry Mouth? Systematic Review and Meta-Regression Analysis of Prevalence Estimates. Braz Dent J 2018;29(6):606-18.
- Liu B, Dion MR, Jurasic MM, Gibson G, Jones JA. Xerostomia and salivary hypofunction in vulnerable elders: prevalence and etiology. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 2012;114(1):52-60.
- Cohen-Brown G, Ship JA. Diagnosis and treatment of salivary gland disorders. Quintessence Int 2004;35(2):108-23.
- Mese H, Matsuo R. Salivary secretion, taste and hyposalivation. J Oral Rehabil 2007;34(10):711-23.
- Miranda-Rius J, Brunet-Llobet L, Lahor-Soler E, Farre M. Salivary secretory disorders, inducing drugs, and clinical management. Int J Med Sci 2015;12(10):811-24.
- Dawes C, Pedersen AM, Villa A, et al. The functions of human saliva: A review sponsored by the World Workshop on Oral Medicine VI. Arch Oral Biol 2015;60(6):863-74.
- Turner MD, Ship JA. Dry mouth and its effects on the oral health of elderly people. J Am Dent Assoc 2007;138 Suppl:15S-20S.
- Eyigor S. Dysphagia in rheumatological disorders. World Journal of Rheumatology 2013;3(3):45-50.
- Parisis D, Chivasso C, Perret J, Soyfoo MS, Delporte C. Current state of knowledge on primary Sjögren's Syndrome, an autoimmune exocrinopathy. Journal of Clinical Medicine 2020;9(7):2299.
- Tan ECK, Lexomboon D, Sandborgh-Englund G, Haasum Y, Johnell K. Medications that cause dry mouth as an adverse effect in older people: a systematic review and metaanalysis. Journal of the American Geriatrics Society 2018;66(1):76-84.
- U.S. Food and Drug Information. Dry mouth? Don't delay treatment. Consumer Health Information. https://www.drugs.com/fda-consumer/dry-mouth-don-t-delay-treatment-183.html . Accessed April 20, 2023.
- Navazesh M, Kumar SK. Xerostomia: prevalence, diagnosis, and management. Compend Contin Educ Dent 2009;30(6):326-8, 31-2; quiz 33-4.
- Ship JA. Diagnosing, managing, and preventing salivary gland disorders. Oral Dis 2002;8(2):77-89.
- Pratt M, Stevens A, Thuku M, et al. Benefits and harms of medical cannabis: a scoping review of systematic reviews. Syst Rev 2019;8(1):320.
- Scully C. Drug effects on salivary glands: dry mouth. Oral Dis 2003;9(4):165-76.
- P.D.Q. Supportive Palliative Care Editorial Board. Oral Complications of Chemotherapy and Head/Neck Radiation (PDQ(R)): Health Professional Version. PDQ Cancer Information Summaries. Bethesda (MD): National Cancer Institute (US); 2002.
- Stein P, Aalboe J. Dental care in the frail older adult: special considerations and recommendations. J Calif Dent Assoc 2015;43(7):363-8.
- Jablonski RY, Barber MW. Restorative dentistry for the older patient cohort. Br Dent J 2015;218(6):337-42.
- Yellowitz JA, Schneiderman MT. Elder's oral health crisis. J Evid Based Dent Pract 2014;14 Suppl:191-200.
- Villa A, Abati S. Risk factors and symptoms associated with xerostomia: a cross-sectional study. Australian Dental Journal 2011;56(3):290-95.
- Zero DT, Brennan MT, Daniels TE, et al. Clinical practice guidelines for oral management of Sjogren disease: dental caries prevention. J Am Dent Assoc 2016;147(4):295-305.
- Brandt JE, Priori R, Valesini G, Fairweather D. Sex differences in Sjögren's syndrome: a comprehensive review of immune mechanisms. Biol Sex Differ 2015 Nov 3;6:19.
- Chiorini JA, Cihakova D, Ouellette CE, Caturegli P. Sjögren syndrome: advances in the pathogenesis from animal models. J Autoimmun 2009;33(3-4):190-6.
- Carr AJ, Ng WF, Figueiredo F, et al. Sjögren's syndrome – an update for dental practitioners. British Dental Journal 2012;213(7):353-57.
- Gordon AJ, Patel A, Zhou F, et al. Minor salivary gland biopsy in diagnosis of Sjögren’s Syndrome. OTO Open 2022;6(3):2473974X221116107.
- Rojas-Ramirez MV, Eldomiaty W, Sangalli L, et al. Xerostomia, reduced salivary flow, and oral burning: associations from a cross-sectional study. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 2023.
- Saleh J, Figueiredo MAZ, Cherubini K, Salum FG. Salivary hypofunction: An update on aetiology, diagnosis and therapeutics. Archives of Oral Biology 2015;60(2):242-55.
- Amorim dos Santos J, Normando AGC, Carvalho da Silva RL, et al. Oral manifestations in patients with COVID-19: a 6-month update. Journal of Dental Research 2021;100(12):1321-29.
- Liu C, Qi X, Yang D, Neely A, Zhou Z. The effects of cannabis use on oral health. Oral Diseases 2020;26(7):1366-74.
- Fox PC, Ship JA. Salivary gland diseases. Burket's Oral Medicine, Diagnosis & Treatment: People's Medical Publishing House USA Ltd (PMPH); 2008. p. 191-222.
- Tanaka A KS. Xerostomia and patients' satisfaction with removable denture performance: systematic review. Quintessence International. 2021 Jan 1;52(1).
- Lynge Pedersen A, Nauntofte B, Smidt D, Torpet L. Oral mucosal lesions in older people: relation to salivary secretion, systemic diseases and medications. Oral Diseases 2015;21(6):721-29.
- Villa A, Wolff A, Narayana N, et al. World Workshop on Oral Medicine VI: a systematic review of medication-induced salivary gland dysfunction. Oral Dis 2016;22(5):365-82.
- Eisai Inc. Salagen (pilocarpine hydrochloride) tablets (rev. 6/2018). " https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=62eda83d-d043-4c7e-8fcf-75d05efbf35b ". Accessed April 20, 2023.
- Daiichi-Sankyo Inc. Evoxac (cevimeline hydrochloride) capsules (rev. 04/2018). " http://www.evoxac.com/ ". Accessed April 20, 2023.
- Han P, Suarez-Durall P, Mulligan R. Dry mouth: A critical topic for older adult patients. Journal of Prosthodontic Research 2015;59(1):6-19.
- OraPharma NeutraSal (supersaturated calcium phosphate) powder for reconstitution. https://pi.bauschhealth.com/globalassets/BHC/PI/NeutraSal-IFU.pdf . Accessed April 20, 2023.
- Chiappelli F. No strong evidence that any topical treatment is effective for relieving the sensation of dry mouth. Evid-based Dent 2012;13(1):16-17.
- Furness S, Worthington HV, Bryan G, Birchenough S, McMillan R. Interventions for the management of dry mouth: topical therapies. Cochrane Database Syst Rev 2011(12):Cd008934.
What products have earned the ADA Seal of Acceptance?
Get a Complete List of ADA-Accepted Products for the Temporary Relief of Dry Mouth
Professional Resources
ADA Council on Scientific Affairs Report: Managing xerostomia and salivary gland hypofunction
ADA Professional Product Review: Palliative Over-the-Counter (OTC) Treatments for Oral Dryness and Inflammation (PDF; pages 21-24)
ADA Oral Health Topics:
Aging and Dental Health
Sjögren Disease
Search JADA for articles related to xerostomia, salivary gland hypofunction, or dry mouth
ADA Library
ADA MouthHealthy:
Medications and Oral Health
Sjögren’s Syndrome
JADA “For the Patient” pages
Is your mouth always dry? (December 2020)
Oral health during cancer treatment (January 2019)
ADA Catalog:
Dry Mouth Patient Brochure (Item #W279)
2016 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria for primary Sjögren's syndrome
American Academy of Oral Medicine: Xerostomia
Mayo Clinic: Dry Mouth
MEDLINE Plus (U.S. National Library of Medicine): Dry Mouth
National Institute for Dental and Craniofacial Research: Dry Mouth
Sjögren's Foundation
Last Updated: April 24, 2023
Prepared by:
Research Services and Scientific Information, ADA Library & Archives.
Content on the Oral Health Topics section of ADA.org is for informational purposes only. Content is neither intended to nor does it establish a standard of care or the official policy or position of the ADA; and is not a substitute for professional judgment, advice, diagnosis, or treatment. ADA is not responsible for information on external websites linked to this website.
- Pathophysiology |
- Evaluation |
- Treatment |
- Geriatrics Essentials |
- Key Points |
Xerostomia is dry mouth caused by reduced or absent flow of saliva.
This condition can result in discomfort, interfere with speech and swallowing, make wearing dentures difficult, cause halitosis , and impair oral hygiene by causing a decrease in oral pH and an increase in bacterial growth. Long-standing xerostomia can result in severe tooth decay and oral candidiasis . Xerostomia is a common complaint among older adults, affecting about 20% of them.
(See also Introduction to the Approach to the Dental Patient .)
Pathophysiology of Xerostomia
Stimulation of the oral mucosa signals the salivatory nuclei in the medulla, triggering an efferent response. The efferent nerve impulses release acetylcholine at salivary gland nerve terminals, activating muscarinic receptors (M 3 ), which increase saliva production and flow. Medullary signals responsible for salivation may also be modulated by cortical inputs from other stimuli (eg, taste, smell, anxiety).
Etiology of Xerostomia
Xerostomia is usually caused by the following:
Radiation to the head and neck (for cancer treatment)
Systemic disorders are less commonly the cause, but xerostomia is common in Sjögren syndrome and may occur in HIV/AIDS , uncontrolled diabetes , and certain other disorders.
Drugs are the most common cause (see table Some Causes of Xerostomia ); about 400 prescription medications and many over-the-counter (OTC) medications cause decreased salivation. The most common include the following:
Anticholinergics
Antiparkinsonian medications
Antineoplastics ( chemotherapeutic agents )
Chemotherapeutic agents cause severe dryness and stomatitis while they are being taken; these problems usually end after therapy is stopped.
Other common drug classes that cause xerostomia include antihypertensives , anxiolytics , and antidepressants (less severe with selective serotonin reuptake inhibitors [SSRIs] than with tricyclics).
The rise of illicit use has resulted in an increasing incidence of meth mouth, which is severe tooth decay and periodontal inflammation bruxing and clenching caused by the drug along with elevated intake of sugary beverages and poor oral hygiene while under the influence of the drug. This combination causes very rapid destruction of teeth.
Tobacco use usually causes a decrease of saliva.
Incidental radiation to the salivary glands during radiation therapy for head and neck cancer often causes severe xerostomia (5200 cGy causes severe, permanent dryness, but even low doses can cause temporary drying).
Evaluation of Xerostomia
History of present illness should include acuity of onset, temporal patterns (eg, constant vs intermittent, presence only on awakening), provoking factors, including situational or psychogenic factors (eg, whether xerostomia occurs only during periods of psychological stress or certain activities), assessment of fluid status (eg, fluid intake habits, recurrent vomiting or diarrhea), and sleeping habits. A history of use of recreational and illicit drugs should be taken.
Review of systems should seek symptoms of causative disorders, including dry eyes, dry skin, rashes, and joint pain ( Sjögren syndrome ).
Past medical history should inquire about conditions associated with xerostomia, including Sjögren syndrome, history of radiation treatment, head and neck trauma, and a diagnosis of or risk factors for HIV infection . Drug profiles should be reviewed for potential offending medications (see table Some Causes of Xerostomia ).
Physical examination
Physical examination is focused on the oral cavity, specifically any apparent dryness (eg, whether the mucosa is dry, sticky, or moist; whether saliva is foamy, thick, stringy, or normal in appearance), the presence of any lesions caused by Candida albicans , and the condition of the teeth.
The presence and severity of xerostomia can be assessed in several ways. For example, a tongue blade can be held against the buccal mucosa for 10 seconds. If the tongue blade falls off immediately when released, salivary flow is considered normal. The more difficulty encountered removing the tongue blade, the more severe the xerostomia. The lipstick sign, where lipstick adheres to the front teeth, may be a useful indicator of xerostomia.
If there appears to be dryness, the submandibular, sublingual, and parotid glands should be palpated while observing the ductal openings for saliva flow. The openings are at the base of the tongue anteriorly for the submandibular and sublingual glands and on the middle of the inside of the cheek for the parotid glands. Drying the duct openings with a gauze square before palpation aids observation. If a graduated container is available, the patient can expectorate once to empty the mouth and then expectorate all saliva into the container. Normal production is 0.3 to 0.4 mL/min. Significant xerostomia is 0.1 mL/min.
Dental caries may be observed at the margins of restorations or in unusual places (eg, at the gum line, incisal edges, or cusp tips of the teeth).
A common manifestation of C. albicans infection is areas of erythema and atrophy (eg, loss of papillae on the dorsum of the tongue). Less common is the better-known white, cheesy curd that bleeds when wiped off.
The following findings are of particular concern:
Extensive tooth decay
Concomitant dry eyes, dry skin, rash, or joint pain
Risk factors for HIV
Interpretation of findings
Xerostomia is diagnosed by symptoms, appearance, and absence of salivary flow when massaging the salivary glands.
No further assessment is required when xerostomia occurs after initiation of a new medication and stops after cessation of that medication or when symptoms appear within several weeks of irradiation of the head and neck. Xerostomia that occurs with abrupt onset after head and neck trauma may be caused by nerve damage.
Concomitant presence of dry eyes, dry skin, rash, or joint pain, particularly in a female patient, suggests a diagnosis of Sjögren syndrome . Severe tooth discoloration and decay, out of proportion to expected findings, may be indicative of illicit drug use, particularly methamphetamines . Xerostomia that occurs only during nighttime or that is noted only on awakening may be indicative of excessive mouth breathing in a dry environment.
Salivary gland biopsy
For patients in whom the presence of xerostomia is unclear, sialometry can be conducted by placing collection devices over the major duct orifices and then stimulating salivary production with citric acid or by chewing paraffin. Normal parotid flow is 0.4 to 1.5 mL/min/gland. Flow monitoring can also help determine response to therapy.
The cause of xerostomia is often apparent, but if the etiology is unclear and systemic disease is considered possible, further assessment should be pursued with biopsy of a minor salivary gland (for detection of Sjögren syndrome , sarcoidosis , amyloidosis , tuberculosis , or cancer ) and HIV testing . The lower lip is a convenient site for biopsy.
Treatment of Xerostomia
Cause treated and causative medications or recreational/illicit drugs stopped when possible
Cholinergic medications
Saliva substitutes
Regular oral hygiene and dental care to prevent tooth decay
When possible, the cause of xerostomia should be addressed and treated.
Patients using continuous positive airway pressure for obstructive sleep apnea may benefit from using the humidifier function of the device. Patients using oral appliance therapy may benefit from a room humidifier.
Symptom control
Symptomatic treatment consists of measures that do the following:
Increase existing saliva
Replace lost secretions
Control caries
Patients should avoid sugary or acidic foods and beverages and any irritating foods that are dry, spicy, astringent, or excessively hot or cold. It is particularly important to avoid ingesting sugar near bedtime.
Treatment reference
1. Chan AKY, Tamrakar M, Jiang CM, et al : Clinical evidence for professionally applied fluoride therapy to prevent and arrest dental caries in older adults: A systematic review. J Dent 125:104273. doi: 10.1016/j.jdent.2022.104273
Geriatrics Essentials: Xerostomia
Although xerostomia becomes more common among older patients, this is probably due to the many medications typically used by those patients rather than aging itself.
Medications are the most common cause, but systemic diseases (most commonly Sjögren syndrome or HIV) and radiation therapy also can cause xerostomia.
Symptomatic treatment includes increasing existing saliva flow with stimulants or medications, and artificial saliva replacement; xylitol-containing gum and sugarless candy may be useful.
Patients with xerostomia are at high risk of tooth decay; meticulous oral hygiene, additional preventive measures in home care, and professionally applied fluorides are essential.

Copyright © 2024 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
- Cookie Preferences

- My presentations
Auth with social network:
Download presentation
We think you have liked this presentation. If you wish to download it, please recommend it to your friends in any social system. Share buttons are a little bit lower. Thank you!
Presentation is loading. Please wait.
To view this video please enable JavaScript, and consider upgrading to a web browser that supports HTML5 video
XEROSTOMIA Physiology, Etiology, Epidemiology, Pathogenesis, Diagnosis, and Treatment Reviewed by:
Published by Edgar Schwartz Modified over 9 years ago
Similar presentations
Presentation on theme: "XEROSTOMIA Physiology, Etiology, Epidemiology, Pathogenesis, Diagnosis, and Treatment Reviewed by:"— Presentation transcript:

© Food – a fact of life 2009 Development and Maintenance of Healthy Teeth Extension.

Seniors Oral Health. Seniors Oral Health Introduction Maintaining healthy teeth and gums at any age is an important part of preserving your overall good.

Medical University of South Carolina/SC-Geriatric Education Center Oral Physiology MSc Students

PowerPoint Presentation to accompany Hole’s Human Anatomy and Physiology, 9/e by Shier, Butler, and Lewis.

NOTES: The Digestive System (UNIT 8, part 1)

Presented by: Cheryl Ann Peters. * A chronic, systemic and inflammatory autoimmune disease in which immune cells attack and destroy exocrine glands that.

Saliva It is the watery fluid produced in the mouths of humans that is produced by the salivary glands , and is made up mainly of water, electrolytes,

Defined as the subjective sensation of oral dryness associated with the reduction or absence of saliva output. Xerostomia is a common problem, not a disease.

ORAL CAVITY SALIVA SECRETION SWALLOWING

Dry Mouth and Related Oral Conditions John T. Frey, D.D.S. How To Dance in the Rain Conference Grand Rapids, MI ◊ September 6, 2014.

SALIVA (Composition and Functions) BY. Dr. Shahzadi Tayyaba Hashmi DNT 353.

Oral Cavity and Pharynx

Salivary Glands Prof. Dr. Thanaa Saad El-Din.

1 Salivary Glands. 2 MAJOR SALIVARY GLANDS SUPPLY SECRETION TO THE ORAL CAVITY Serous Glands- secrete serum (which is a clear liquid 90% water) Mucous.

REQUIREMENTS Adequate lighting Two dental mouth mirrors Gloves

Introduction and Physiological anatomy of Gastro Intestinal tract Every cell of living system needs energy Unicellular organisms: Exists in the sea of.

Dentistry The Teeth, Gums, and Mouth Wesley S. Mullins, D.D.S. November 23, 2004.

“You cannot be healthy without oral health.” Surgeon General’s Report on Oral Health ~May WDSF 2011 ©

Histology of Glands Dr. Archana Rani Associate Professor

BIOLOGY OF THE HUMAN DENTITION
About project
© 2024 SlidePlayer.com Inc. All rights reserved.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Ann Med Health Sci Res
- v.4(4); Jul-Aug 2014
Xerostomia Due to Systemic Disease: A Review of 20 Conditions and Mechanisms
H mortazavi.
1 Department of Oral and Maxillofacial Medicine, Dental School, Shahid Beheshti University of Medical Sciences, Tehran, Iran
M Baharvand
A movahhedian.
2 Dental Student, Shahid Beheshti University of Medical Sciences, Tehran, Iran
M Mohammadi
A khodadoustan.
3 Periodontist, Private Practice, Tehran, Iran
Xerostomia is a common complaint of nearly half of the elderly population and about one-fifth of younger adults. It causes several signs and symptoms, and compromise oral functions and health-related quality-of-life. Multiple reasons are proposed to describe the etiology of xerostomia such as local factors, psychogenic factors, and systemic diseases. In order to manage xerostomia effectively, identification of the main causality is mandatory. The aim of this review was to present systemic diseases leading to xerostomia with their mechanisms of action. We used various general search engines and specialized databases such as Google, Google Scholar, Yahoo, PubMed, PubMed Central, MedLine Plus, Medknow, EBSCO, ScienceDirect, Scopus, WebMD, EMBASE, and authorized textbooks to find relevant topics by means of Medical Subject Headings keywords such as “xerostomia,” “hyposalivations,” “mouth dryness,” “disease,” and “systemic.” We appraised 97 English-language articles published over the last 40 years in both medical and dental journals including reviews, meta-analysis, original papers, and case reports. Upon compilation of relevant data, it was concluded that autoimmune diseases most frequently involve salivary glands and cause xerostomia followed by diabetes mellitus, renal failure, and graft-versus-host disease. Moreover, the underlying mechanisms of systemic disease-related xerostomia are: autoimmunity, infiltration of immunocompetent cells, granuloma formation, fibrosis and dehydration, deposition of proteinaceous substances, bacterial infection, and side-effects of medications.
Introduction
Xerostomia is the subjective complaint of oral dryness, while salivary gland hypofunction is an objective matter characterized by reduced salivary flow.[ 1 ] These two terms are often incorrectly used interchangeably.
Xerostomia is a frequent annoying condition. It is estimated that 12-47% of the elderly and 10-19.3% of people in their early 30's have been suffering from dry mouth.[ 2 , 3 , 4 ] The symptoms of xerostomia are as follows: Cracked peeled atrophic lips, glossitis, progressive cervical, or cusp tip caries even with optimum oral hygiene, candidiasis, and pale corrugated dry buccal mucosa. The size, texture and tenderness of salivary glands should be assessed. Xerostomia can lead to dysphagia, dysgeusia, oral pain, dental caries, oral infection, periodontal disease, and finally can affect the health-related quality-of-life.[ 5 , 6 , 7 , 8 ] Malnutrition and psychosocial problems could be associated with dry mouth as well.[ 8 ] The basis of xerostomia is the alteration in both quantitative and qualitative function of salivary glands.[ 6 ] There are multiple causes with various mechanisms of xerostomia such as systemic diseases, anticholinergic effects of many drugs, psychological conditions, alcohol, head and neck radiation therapy, and physiological changes, but xerostomia-related systemic diseases have not been addressed as much as they worth it.[ 9 ] In order to better understanding, diseases which cause xerostomia, the underlying mechanisms and the incidence or prevalence of dry mouth due to systemic conditions are summarized in Tables Tables1 1 and and2. 2 . Multiple methods have been described to manage xerostomia. Saliva substitutes, topical stimulants, and parasympathetic agonists such as pilocarpine and cevimeline are approved medications to treat xerostomia.[ 10 ] Early detection of these diseases may aid to timely treatment of xerostomia. Some of these systemic conditions are so severe that distract the attention of health care workers away from the complications such as xerostomia, which might cause additional discomfort for the patient.
Mechanisms of xerostomia due to systemic diseases

Incidence or prevalence of xerostomia due to systemic diseases

The aim of this study was to describe systemic diseases leading to xerostomia to provide physicians and dentists with an update and comprehensive source for their clinical practice.
Methods of Literature Search
We used various general search engines such as Google, Google Scholar, and Yahoo as well as bibliographic databases such as PubMed, PubMed Central, Medline Plus, Medknow, EBSCO, ScienceDirect, Scopus, WebMD, EMBASE, and three authorized textbooks to find relevant topics by means of medical subject headings keywords such as “xerostomia,” “hyposalivations,” “mouth dryness,” “disease,” and “systemic.” The search was accomplished in 2013 and limited to English-language articles published over the last 40 years in both medical and dental journals. Totally, 258 articles were identified. After provisional assessment of the titles and abstracts by two reviewers, 106 articles were found to be relevant to the topic, and out of them 97 were available for us including 20 reviews and meta-analysis, 59 original papers, and 18 case reports regarding systemic disease resulting to xerostomia. Our review included articles published between 1997-2013, in the years of 1974, 1980, 1983, 1987, 1989, and 1990.
After compilation of information from relevant articles and updated textbooks, we categorized systemic diseases resulting in xerostomia to endocrine diseases, viral infections, bacterial infections, autoimmune diseases, granulomatous diseases, storage diseases, and some other unclassified diseases as follows. Meanwhile, the underlying mechanisms of xerostomia due to systemic diseases, and the incidence or prevalence of xerostomia in each disease were summarized in Tables Tables1 1 and and2 2 .
Endocrine diseases
Diabetes mellitus.
Diabetes mellitus is an endocrine disease characterized by the deficit in production of insulin with consequent alteration of metabolism and balance of glucose concentration. According to its etiology, it is classified as Type 1 and 2.[ 11 ] Type 1 diabetes mellitus is a metabolic dysfunction characterized by hyperglycemia resulting from definite shortage of insulin secretion caused by autoimmune illness and genetic factors.[ 12 ] Type 2 diabetes mellitus (formerly known as non-insulin-dependent diabetes mellitus) is the most common form of disease featured by hyperglycemia, insulin resistance, and relative insulin deficiency. Type 2 diabetes results from interaction between genetic, environmental and behavioral risk factors.[ 13 ] It is estimated that there will be 380 million persons with diabetes mellitus in 2025.[ 14 ]
Patients with uncontrolled diabetes often report dry mouth, which is believed to be due to polyuria, dehydration, and autonomic dehydration.[ 11 ] The prevalence of xerostomia was reported in 14-62% of diabetes mellitus 2 cases,[ 15 , 16 , 17 ] and it was found in 38.5% and 53% of children and adolescents subjects with diabetes mellitus 1, respectively.[ 17 , 18 ]
Thyroid disease
Autoimmune thyroid disease, including Graves’ disease and Hashimoto's thyroiditis, is one of the most common immune-mediated conditions.[ 19 ] Autoimmune thyroid disease is characterized by the presence of serum antibodies against thyroid-specific or thyroid-restricted antigens like the thyroid stimulating hormone receptor, thyroperoxidase, and thyroglobulin).[ 20 ] The prevalence of autoimmune thyroid disease in the general population varies among countries. Prevalence has been estimated as 5-15% in women and 1-5% in men. In other words, autoimmune thyroid disease can be regarded as the most common autoimmune endocrine disease.[ 21 ] A considerable number of patients with primary Sjögren's syndrome (pSS) along with thyroid disease diagnosed by laboratory data and clinical presentation were reported.[ 22 ] The coexistence of Sjögren's syndrome and thyroiditis is frequent suggesting a common genetic or environmental predisposing factor with similar pathogenic mechanisms. pSS was reported to be 10 times more frequent in patients with autoimmune thyroid disease, while autoimmune thyroiditis was 9 times more frequent in pSS. Therefore, Sjögren's syndrome should be studied in patients with thyroid disease and vice versa.[ 23 ]
Viral infections
Human immunodeficiency virus.
Human immunodeficiency virus (HIV) infection is one of the most devastating infections in modern times. Oral manifestations of HIV infection occur in approximately 30-80% of patients.[ 24 ] Oral lesions are among the early signs of HIV infection and can predict progression to acute immunodeficiency syndrome. The more common HIV-related lesions include oral candidiasis, herpes simplex infection, oral Kaposi's sarcoma, oral hairy leukoplakia, parotid gland enlargement, periodontal diseases (linear gingival erythema and necrotizing ulcerative periodontitis), human papilloma virus-associated warts, and ulcerative conditions including herpes simplex virus lesions, recurrent aphthous ulcers, neutropenic ulcers, and xerostomia.[ 25 , 26 ] Xerostomia is due to the side effects of HIV medications (e.g., didanosine) or the proliferation of CD8 + cells in the major salivary glands.[ 26 ] Parotid hypertrophy as a compensative reaction has been also found more commonly in HIV-positive children.[ 27 , 28 ] Xerostomia has been estimated as 1.2-40% in HIV-positive patients.[ 26 , 29 , 30 , 31 , 32 , 33 ] Although the role of HIV on xerostomia is relatively clear, there is a controversy about xerostomia prevalence as demonstrated by Sontakke et al ., Pinheiro et al ., and Nittayananta et al .[ 32 , 33 , 34 ] There is another conflict about xerostomia-related HIV medications in the literature, for example Lin claimed that xerostomia was not compounded by medications.[ 35 ] In contrast, some researchers believe that taking anti-HIV drugs is effective on the prevalence of xerostomia.[ 26 , 32 ]
Hepatitis C virus
The hepatitis C virus (HCV) is a linear, single-stranded RNA virus of the Flaviviridae family that was first identified in 1989.[ 36 ] HCV infection is a major health problem among the general population, and its extrahepatic manifestations have also been reported like Sicca syndrome.[ 37 ] Several autoimmune and immune complex-mediated disorders have been proposed to be related to HCV infection such as essential mixed cryoglobulinemia, which is frequently associated with Sjögren's syndrome. The association between HCV and Sjögren's syndrome may be related to the following reasons: (1) close association between HCV infection and mixed cryoglobulinemia, (2) the salivary gland tropism of HCV.[ 38 ] However, some studies did not find any relationship between xerostomia and the presence of HCV infection.[ 39 , 40 ] Xerostomia has been found among 5-55% of HCV-infected patients.[ 36 , 38 , 39 , 41 , 42 ] Xerostomia is also an adverse event during ribavirin-interferon therapy.[ 43 , 44 ]
Epstein-Barr virus
Epstein-Barr virus (EBV) is a human herpes virus that establishes long-term latent infection in B-lymphocytes named EBV infectious mononucleosis (EBV-IM).[ 45 ] EBV-IM is a common infection that affects 25-30% of adolescents and adults up to 30 years of age.[ 46 ] Association between EBV and autoimmune diseases, such as rheumatoid arthritis (RA), systemic lupus erythematosus, multiple sclerosis, autoimmune thyroiditis, inflammatory bowel diseases, insulin-dependent diabetes mellitus, systemic sclerosis, myasthenia gravis, autoimmune liver diseases, and Sjögren's syndrome have been suggested.[ 47 ] It is proposed that the initiating event in pSS is an infection with EBV, and the autoimmune exocrinopathy that progresses to keratoconjunctivitis Sicca and xerostomia is sequelae to this process. It is noted that during EBV infection, there are multiple copies of the EBV-encoded small RNAs available to bind to the La ribonucleoprotein and when infection occurs in subjects who are genetically predisposed to autoimmunity and have an impaired T-cell-mediated response to EBV, there is a loss of immunological tolerance to La with production of anti-La (SS-B). Thus the inflammatory process in exocrine glands, which culminates in the Sicca syndrome is due to the combined effects of chronic EBV infection and autoimmunity. The mean titer of anti-EBV nuclear-antigen antibodies was significantly higher in Sjögren's syndrome patients than in normal people.[ 48 ]
Cytomegalovirus
Cytomegalovirus (CMV) is a common infection with a seroprevalence among adolescents ranging from 47% to 89%.[ 49 ] The persistence of CMV with alteration of cell surface expression in certain tissues may initiate the tissue destruction that leads to the clinical manifestations of Sjögren's syndrome. Ductal cells of salivary and lacrimal glands are immunologically attacked due to CMV antigenic expression. The destruction of these ducts leads to xerostomia.[ 50 ] However, no relationship between xerostomia and anti-CMV antibodies was noted.[ 51 ]
Human T-lymphotropic virus type 1
Human T-lymphotropic virus Type 1 (HTLV-1) is known to cause HTLV-associated myelopathy (HAM)/tropical spastic paraparesis and adult T-cell leukemia.[ 52 ] It is estimated that 15-20 million persons are currently infected with HTLV-1 worldwide.[ 53 ]
Retroviruses such as HTLV-1 and HIV infect immunocompetent cells, resulting in the destruction or overstimulation of T-cells, and act as potential triggers for autoimmune disease.[ 54 ]
Previous studies reported a high prevalence rate of anti-HTLV-1 antibodies in the peripheral blood in 3.8-36.7% of patients with Sjögren's Syndrome.[ 55 , 56 , 57 , 58 ]
Bacterial infections
Actinomycosis.
Actinomycosis is an anaerobic bacterial infection affecting men more frequently between the ages of 30-60 years. Almost half of actinomycosis cases occur in the cervicofacial region, and salivary glands may be involved as well. The organism can colonize inside the ducts of both submandibular and parotid glands and leads to abscess formation in the submandibular and masseter spaces, respectively.[ 59 , 60 , 61 ]
Autoimmune diseases
Rheumatoid arthritis.
Rheumatoid arthritis is a systemic disease of connective tissue origin, which affects 1% of the world population. Women have a 3-fold higher incidence than do men. RA frequently presents with extra-articular features such as hematologic, neurologic, and cardiovascular involvement concomitant with dysfunction of lacrimal and salivary glands. Zalewska et al . showed impairment of salivary immunity system of the oral cavity in xerostomic patients with RA.[ 62 ] Secondary Sjögren's syndrome is associated with xerostomia and occurs with autoimmune diseases most frequently with RA.[ 63 ]
Systemic lupus erythematosus
Systemic lupus erythematosus (SLE) is an inflammatory connective tissue disease with characteristic autoantibodies. SLE is much more common in women than men. It may occur at any age, but appears most often in people between the ages of 10 and 50. More than 75% of patients with SLE are affected with xerostomia. Coexistence of Sjögren's syndrome and SLE has been found in 1/3 of SLE patients. SLE has been shown to be associated with a decreased unstimulated salivary flow rate.[ 64 ]
Primary biliary cirrhosis
Primary biliary cirrhosis (PBC) is a cholestatic autoimmune disease predominantly of middle-aged women with progressive destruction of interlobular bile ducts.[ 65 ] The most autoimmune disease in PBC patients is Sjögren's syndrome[ 66 ] whose symptoms have been observed in 47-73% of patients[ 67 , 68 ] Xerostomia as well as dysphagia seems to be associated with PBC.[ 69 ]
Scleroderma
Progressive systemic sclerosis or scleroderma is a chronic sclerotic disease with deposition of extracellular matrix throughout connective tissue and vascular abnormalities, which leads to tissue hypoxia.[ 70 ] Fibrosis of capillaries, excretory ducts and acini of salivary and lacrimal glands are associated with xerostomia as oral manifestations of scleroderma.[ 71 ] Lymphocytic infiltration has been observed among 15% of patients with systemic sclerosis, which is a sign of secondary Sjögren's syndrome.[ 72 ]
Granulomatous diseases
Sarcoidosis.
Sarcoidosis is a systemic inflammatory disease with unknown etiology characterized by the presence of noncaseating granulomas that can affect any organ (mostly lungs and lymph nodes).[ 73 ] Coexistence of parotid and submandibular gland swelling and xerostomia has been reported in sarcoidosis patients.[ 74 , 75 , 76 ] Mansour et al ., identified five patients representing both clinical and histological features of Sjögren's syndrome and sarcoidosis, suggesting inclusion of sarcoidosis as diagnostic criteria for Sjögren's syndrome.[ 74 ]
The salivary glands could be affected by sarcoidosis as well, which was reported in 6% of the cases. Parotid salivary gland enlargement was also detected in 6% of the patients.[ 74 ] Parotid gland enlargement in patients presenting with Sicca symptoms is believed to be of clinical significance. Such finding might be more likely associated with sarcoidosis, especially in patients presenting with negative serologic profiles.[ 74 ]
Tuberculosis
Tuberculosis (TB) is a chronic bacterial infection, caused by Mycobacterium TB leading to formation of granulomas in infected tissues. The lungs are most commonly affected, but other tissues, including the salivary glands, may be involved. Patients with TB may experience xerostomia and/or salivary gland swelling, with granuloma or cyst formation within the affected glands. Salivary gland enlargement usually presents as part of a characteristic symptom complex, however salivary gland changes have been reported in the absence of systemic symptoms.[ 77 ]
Granulomatous diseases such as sarcoidosis and TB may cause salivary gland hypofunction and lead to xerostomia.[ 78 ]
Storage diseases
Hemochromatosis.
Hemochromatosis is defined as a pathological condition with iron overload in vital organs with a hereditary/primary cause.[ 79 ] Organs commonly affected by hemochromatosis are liver, heart, and endocrine glands. Iron deposition in salivary glands causes hyposalivation. Patients with normal ferritin level had normal salivary flow rate, whereas those with high levels of ferritin showed decreased stimulatory salivary flow rate.[ 79 , 80 ]
Amyloidosis
Amyloidosis is characterized by deposition of an extracellular protein-like material called amyloid. Amyloidosis causes various effects on different organs with a variety of extensions. In addition, amyloidosis may be associated with multiple myeloma or chronic infections. Amyloidosis may be accompanied with oral involvement in the form of macroglossia (10-40%), oral amyloid nodules, and dry mouth due to amyloid infiltration and destruction of salivary glands.[ 81 ] A case of pSS manifested as localized cutaneous nodular amyloidosis has been reported.[ 82 ] Meanwhile, a relationship between amyloidosis and xerostomia has been documented.[ 82 , 83 , 84 ]
End-stage renal disease
End-stage renal disease (ESRD) represents a clinical state or condition with irreversible loss of the endogenous renal function to a degree, which is sufficient to render the patient permanently dependent upon renal replacement therapy in the form of dialysis or kidney transplantation. ESRD leads to accumulation of certain toxic elements, which affects normal functions of the body, and may have significant complications including cardiovascular disease, immune deficiency, anemia, renal function impairment, and bone disease.[ 85 ] Xerostomia was found in 28-59% of ESRD patients due to inability of kidneys to reabsorb sodium and the resultant polyuria.[ 86 , 87 ]
Ectodermal dysplasia
Ectodermal dysplasia is a hereditary disease causing anomalies in tissues of ectodermal origin. The significance of this disease lies in severe hypodontia, and an accompanying hypoplasia of the alveolar process. The clinical condition is aggravated by a significant xerostomia as a result of salivary gland aplasia or hypoplasia.[ 88 , 89 ] However, in some patients with ectodermal dysplasia with the presence of salivary glands, hyposalivation have been reported. In a study of 39 patients with ectodermal dysplasia, salivary flow rate was decreased in 13 (33.3%) patients.[ 90 ]
Hematopoietic stem cell transplantation and chronic graft-versus-host disease
Chronic graft-versus-host disease (cGVHD) is a multi-organ involvement that occurs post hematopoietic stem cell transplantation (HSCT), with the mouth being one of the most frequently affected sites.[ 91 ] The pathogenesis of GVHD is based on donor graft T-lymphocytes that recognize antigenic disparities between donor and recipient and the dysregulation of a broad panel of cytokines. GVHD occurs in 40-70% of patients treated by bone marrow and peripheral blood stem cell transplantation.[ 92 ] Oral manifestations are common in patients diagnosed with chronic graft-versus-host-disease.[ 91 ] Hull et al . mentioned xerostomia as the most common oral symptom in patients with history of HSCT with the majority of patients (53%) having clinical markers of oral cGVHD.[ 93 ] Noce et al . reported that 59.1% of patients diagnosed with cGVHD had salivary gland dysfunction.[ 91 ] Boer et al . showed a decrease in salivary flow rate (16% of patients) and a relation between hyposalivation intensity and elapsed time after HSCT.[ 94 ] There is similarity in oral clinical manifestations of GVHD and Sjögren's Syndrome because of the same autoimmune nature, but differences have also been found.[ 95 ] The suggested pathophysiological mechanisms of xerostomia and hyposalivation observed in GVHD are lymphocytic infiltration, parenchymal destruction, and fibrosis within salivary gland tissue.[ 95 ]
Parkinson's disease
Parkinson's disease (PD) is a relatively common, progressive, debilitating, and neurological disorder. Cardinal symptoms are resting tremor, bradykinesia, akinesia, restricted mobility, and postural instability. Levodopa (L-DOPA) has been used as a primary drug for over 30 years. L-DOPA is converted into dopamine in the dopaminergic neurons by DOPA decarboxylase enzyme. Proulx et al . have reported that patients with PD produce less saliva than normal. Factors influencing the production of saliva include the use of levodopa and female gender.[ 96 ] Hyposialorrhea is an early autonomic manifestation of PD.[ 97 ]
Salivary glands are involved due to many systemic diseases with the resultant complication of xerostomia. Autoimmune diseases, diabetes mellitus, ESRD, and GVHD are frequently associated with salivary hypofunction. The underlying mechanism of xerostomia differs in terms of disease. Autoimmunity accounts for xerostomia related to SLE, RA, PBC, thyroid disease, and some viral infections. Some conditions affect salivary glands through infiltration of immunocompetent cells or granuloma formation such as HIV infection, GVHD, sarcoidosis, and TB. Polyuria and dehydration is responsible for dry mouth associated with diabetes and end-stage renal failure, while GVHD and scleroderma cause xerostomia because of fibrosis. Deposition of proteinaceous substances and bacterial infection are also mentioned as alternative mechanisms for xerostomia. Identification of the main reason of xerostomia helps attain timely diagnosis and more appropriate treatment plan.
Source of Support: Nil.
Conflict of Interest: None declared.
LOG IN | NOT A MEMBER? REGISTER FREE!
- Dental Assistant
- Live Webinars
- On-Demand Webinars
- DEA Opioid Modules
- American Dental Assistants Association
- ClearCorrect
- Inside Dental Assisting
- Inside Dental Hygiene
- Inside Dental Technology
- Inside Dentistry
- PDS UNIVERSITY – INSTITUTE OF DENTISTRY
- United Concordia Dental Insurance
- Tufts University
CDEWorld > Courses > Xerostomia: Prevalence, Diagnosis, and Management
View the digital edition, learning objectives:.
After reading this article, the reader should be able to:
- define xerostomia and salivary gland hypofunction.
- know the prevalence and causes, especially in the elderly.
- describe the diagnostic work-up and various management options available for elderly patients.
Disclosures:
The author reports no conflicts of interest associated with this work.
Xerostomia: Prevalence, Diagnosis, and Management
Mahvash navazesh, dmd; satish k. s. kumar, mdsc, july/august 2009 issue - expires friday, august 31st, 2012, compendium of continuing education in dentistry.
This article summarizes the common causes, clinical presentation, and complications of xerostomia and salivary gland hypofunction in the geriatric population and discusses the various management options.
You must be signed in to read the rest of this article.
Login Sign Up
Registration on CDEWorld is free. Sign up today! Forgot your password? Click Here !
Today, life expectancy in the US has been estimated to have reached a record high of 77.8 years. The percentage of the population that is 75 years of age and older was 6% in 2005 and projected to double to 12% by 2050. While longer life expectancy is attributable to advances in healthcare, the prevalence of age-related chronic diseases and conditions will increase. From 2004 to 2005, the percentage of older adults with limited activity levels ranged from 25% among 65- to 74-year-olds to 60% of adults 85 years and older. Arthritis and other musculoskeletal conditions were the most common chronic medical morbidities that reduced activity in older individuals, followed by heart and circulatory problems. The percentage of adults with three or more ongoing conditions increased with age from 7% of those who are 45 to 54 years of age to 37% of people 75 years and older. 1 Obviously, medication intake is higher with these chronic conditions, several of which are associated with dry mouth and related complications. 2-5 This article will summarize the etiology, diagnosis, and management of xerostomia and salivary gland hypofunction, with emphasis on the elderly.
Xerostomia is a symptom defined as dry mouth, which may be associated with objective evidence of salivary gland hypofunction. A patient is considered to have reduced salivary flow if the unstimulated salivary flow is ≤ 0.1 mL/min measured for 5 to 15 minutes or if the chewing-stimulated salivary flow is ≤ 0.7 mL/min measured for 5 minutes. 6-9
The prevalence of xerostomia in the general population is unclear because of the scant number of studies. Reports of the prevalence vary, ranging from 0.9% to 64.8%. 10 The incidence of xerostomia increases from 6% at 50 years of age to 15% at 65 years of age. 11 One finding estimated the occurrence of xerostomia in people 65 years and older to be approximately 30%. 12 However, the prevalence reaches almost 100% in patients with Sjögren’s syndrome and those who are receiving radiation therapy for head and neck cancer. 12
Aging per se has no significant impact on salivary gland secretion. 12 In the elderly, several factors, such as decrease of ptyalin, increase of mucin, and low stimulation of the peripheral receptors, have been implicated in xerostomia. 13 Xerostomia and/or salivary gland hypofunction in this population has been associated with a number of systemic disorders (Table 1) and medications 14,15 (Table 2). The incidence increases with medication exposure, 16 with more than 400 drugs implicated. 2 In a 5-year longitudinal study, the relationship of dry mouth and long-term exposure to medications was assessed. Xerostomia severity was found to be higher among females and associated with the use of medications, such as antianginal, diuretics, antidepressants, and antiasthma, as well as thyroxine. 17 Xerostomia and salivary gland hypofunction are also major complications of radiation or chemotherapy. Long-term morbidity in patients receiving combined radiation and chemotherapy is significant because of xerostomia, salivary gland hypofunction, and severe dysphagia. 18

Clinical Presentation and Complications
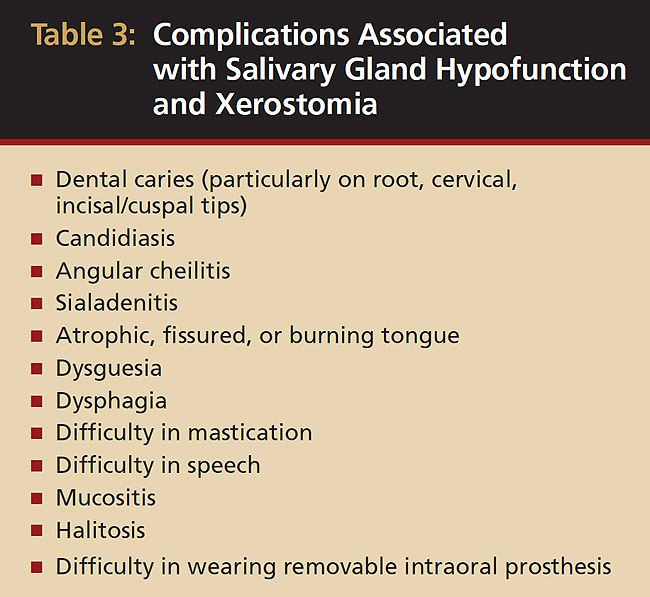
Saliva aids for oral cavity cleansing, swallowing, taste, speech, and digestion could be compromised in patients with salivary gland hypofunction. The oral mucosa may appear dry and friable. The tongue may appear dry and fissured ( Figure 1 ). Dental caries, plaque accumulation, gingivitis, and periodontitis are common in patients with significant salivary gland hypofunction ( Figure 2 ). Infections, such as oral candidiasis ( Figure 3 ), and enlargement of salivary glands from sialadenitis are seen commonly in patients with moderate-to-severe salivary gland hypofunction ( Figure 4 ). Difficulty in mastication and swallowing also may indicate advanced salivary gland hypofunction 19 and can contribute to poor nutrition. 20 Denture retention may become difficult because of the lack of saliva 12 (Table 3).
Oral healthcare providers can use a simple diagnostic algorithm to identify patients at risk of developing these problems 21 and measure salivary flow rates for an objective assessment. 22 Clinicians can use a simple questionnaire to assess dry mouth. A “yes” response to the following four questions has been associated with salivary gland hypofunction: 9
- Does the amount of saliva in your mouth seem too little?
- Does your mouth feel dry when eating a meal?
- Do you have difficulty swallowing any food?
- Do you sip liquids to aid in swallowing dry food?
Visual analog scales and/or an ordinal scale based on ranked categories (eg, I have no/slight/severe/annoying feeling of dry mouth) also may be used. 23 Objective measurements of both qualitative and quantitative changes in saliva are best performed by saliva collection from individual glands or all glands as reflected in whole saliva. 22
A thorough medical history that includes the patient’s use of medications followed by clinical examination is necessary to establish a diagnosis. Further tests such as serologic evaluations (antinuclear antibodies, eg, rheumatoid factor, anti-Ro/anti-SS-A, anti-La/anti-SS-B), minor salivary gland biopsy (for detection of lymphocytic infiltration to eliminate systemic diseases, such as Sjögren’s syndrome or drug-induced sialadenitis), salivary gland imaging such as sialography and scintigraphy, and sialometric evaluations may be required to confirm the diagnosis and to determine any underlying systemic conditions. Consultation with physicians is critical to discuss if the medication responsible for xerostomia can be reduced in dosage or substituted with one that has little or no salivary side effects.
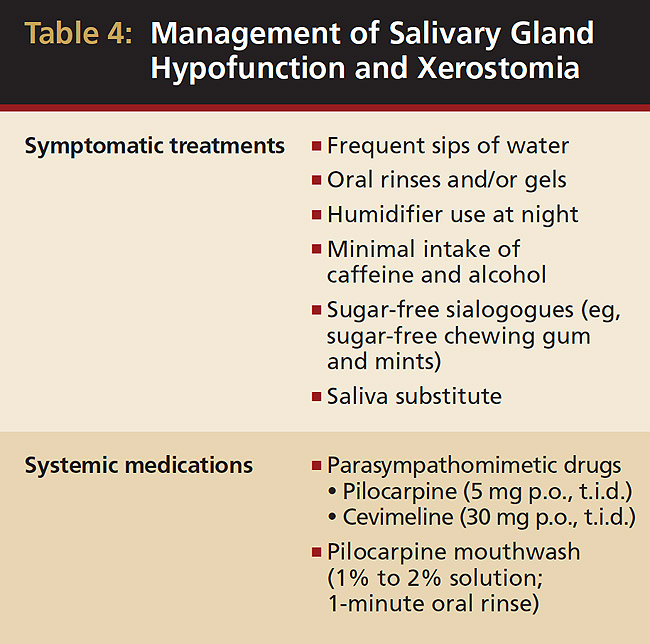
After determining a diagnosis and possible underlying causes, dental clinicians should begin management of these patients according to the severity of the condition. Symptomatic or palliative treatment of xerostomia, although transient, has proven to be beneficial and patient compliance is good (Table 4). Frequent sips of water as well as alcohol-free oral rinses, gels, mouthwashes, sugar-free chewing gum, and mints have all proven useful in reducing the feeling of dry mouth. Because xerostomia typically feels worse at night, use of a humidifier at night is helpful. Avoiding dehydration by minimizing caffeine and alcohol intake is recommended. Artificial saliva is typically not well-liked by patients and does not last. 24 Severe salivary gland hypofunction and associated xerostomia can be managed by generalized parasympathomimetics, such as pilocarpine HCI (SALAGEN®, Pharmacia, Saint Paul, MN). However, the side effects of that medication, such as sweating, vasodilation, headaches, and urinary frequency, can decrease patient compliance. 25 Cevimeline HCI (EVOXAC®, Daiichi Sankyo Inc., Tokyo, Japan) is another drug approved by the Food and Drug Administration (FDA) for treatment of oral dryness in Sjögren’s syndrome and administered as 30 mg, p.o., t.i.d. 3,26 Pilocarpine HCI has been shown to be effective when used as a mouthwash for 1 minute in healthy individuals. This has shown to increase objective salivary flow (with 1% and 2% concentrations) and subjective salivary flow (with 2% concentration). 27 Amifostine (Ethyol®, ALZA Corporation, Mountain View, CA) is effective in patients receiving radiotherapy. 28 Amifostine is a thiol drug that is cytoprotective by several mechanisms, including scavenging oxygen-derived free radicals, deoxyribonucleic acid protection and repair acceleration, and induction of cellular hypoxia. The medication has FDA approval to reduce the incidence of moderate-to-severe xerostomia in patients undergoing postoperative radiation treatment for head and neck cancer. 29-31
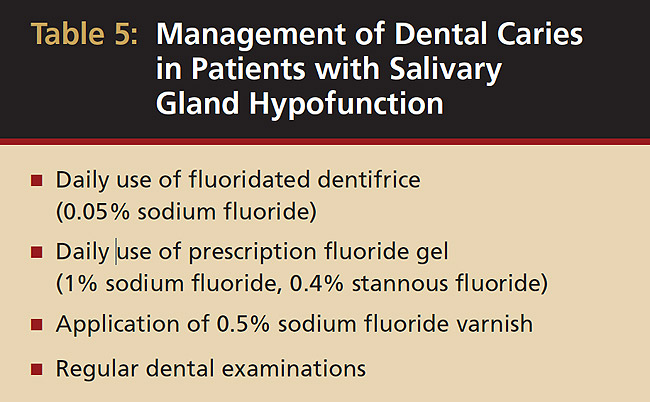
Fluorides, remineralizing solutions, and a noncariogenic diet are critical for preventing dental caries (Table 5). Regular dental examinations should be every 2 to 6 months, based on risk factors and disease susceptibility, such as past caries experience, periodontal status, quantity and quality of saliva, and disabling conditions that prevent oral hygiene maintenance.
The elderly population is expanding and so too are the rates of medical conditions and medication uses. This potentially may increase the prevalence of xerostomia and salivary gland hypofunction. Familiarity with contributing factors, clinical manifestations, and complications associated with xerostomia will help in better management. Preventive approaches will enhance quality of life in the elderly, who are more likely to have xerostomia.
1. Health, United States, 2007. Department of Health and Human Services, United States. http://www.cdc.gov/nchs/data/hus/hus07.pdf. Accessed February 10, 2009.
2. Sreebny LM, Schwartz SS. A reference guide to drugs and dry mouth—2nd edition. Gerodontology . 1997;14(1):33-47.
3. von Bültzingslöwen I, Sollecito TP, Fox PC, et al. Salivary dysfunction associated with systemic diseases: systematic review and clinical management recommendations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod . 2007;103(suppl):S57.e1-e15.
4. Moore PA, Guggenheimer J. Medication-induced hyposalivation: etiology, diagnosis, and treatment. Compend Contin Educ Dent . 2008;29(1):50-55.
5. Mulligan R, Sobel S. Drugs commonly used by the elderly: a review for dental practice. J Calif Dent Assoc . 1994;22(3):35-47.
6. Navazesh M, Christensen C, Brightman V. Clinical criteria for the diagnosis of salivary gland hypofunction. J Dent Res . 1992;71(7): 1363-1369.
7. Ship JA, Fox PC, Baum BJ. How much saliva is enough? ‘Normal’ function defined. J Am Dent Assoc . 1991;122(3):63-69.
8. Tylenda CA, Ship JA, Fox PC, et al. Evaluation of submandibular salivary flow rate in different age groups. J Dent Res . 1988; 67(9):1225-1228.
9. Fox PC, Busch KA, Baum BJ. Subjective reports of xerostomia and objective measures of salivary gland performance. J Am Dent Assoc . 1987;115(4):581-584.
10. Orellana MF, Lagravère MO, Boychuk DG, et al. Prevalence of xerostomia in population-based samples: a systematic review. J Public Health Dent . 2006;66(2):152-158.
11. Johansson AK, Johansson A, Unell L, et al. A 15-yr longitudinal study of xerostomia in a Swedish population of 50-yr-old subjects. Eur J Oral Sci . 2009;117(1):13-19.
12. Ship JA, Pillemer SR, Baum BJ. Xerostomia and the geriatric patient. J Am Geriatr Soc . 2002;50(3):535-543.
13. Astor FC, Hanft KL, Ciocon JO. Xerostomia: a prevalent condition in the elderly. Ear Nose Throat J . 1999;78(7):476-479.
14. Navazesh M, Brightman VJ, Pogoda JM. Relationship of medical status, medications, and salivary flow rates in adults of different ages. Oral Surg Oral Med Oral Pathol Oral Radiol Endod . 1996;81(2):172-176.
15. Wu AJ, Ship JA. A characterization of major salivary gland flow rates in the presence of medications and systemic diseases. Oral Surg Oral Med Oral Pathol. 1993;76(3):301-306.
16. Thomson WM, Chalmers JM, Spencer AJ, et al. A longitudinal study of medication exposure and xerostomia among older people. Gerodontology. 2006;23(4):205-213.
17. Thomson WM, Chalmers JM, Spencer AJ, et al. Medication and dry mouth: findings from a cohort study of older people. J Public Health Dent . 2000;60(1):12-20.
18. Nguyen NP, Sallah S, Karlsson U, et al. Combined chemotherapy and radiation therapy for head and neck malignancies: quality of life issues. Cancer . 2002;94(4):1131-1141.
19. Kaplan I, Zuk-Paz L, Wolff A. Association between salivary flow rates, oral symptoms, and oral mucosal status. Oral Surg Oral Med Oral Pathol Oral Radiol Endod . 2008;106(2):235-241.
20. Ritchie CS, Joshipura K, Hung HC, et al. Nutrition as a mediator in the relation between oral and systemic disease: associations between specific measures of adult oral health and nutrition outcomes. Crit Rev Oral Biol Med . 2002;13(3):291-300.
21. Navazesh M, Denny P, Sobel S. Saliva: a fountain of opportunity. J Calif Dent Assoc . 2002;30(10):783-788.
22. Navazesh M, Kumar SK; University of Southern California School of Dentistry. Measuring salivary flow: challenges and opportunities. J Am Dent Assoc . 2008;139(suppl):35S-40S.
23. Pai S, Ghezzi EM, Ship JA. Development of a Visual Analogue Scale questionnaire for subjective assessment of salivary dysfunction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod . 2001;91(3):311-316.
24. Turner MD, Ship JA. Dry mouth and its effects on the oral health of elderly people. J Am Dent Assoc . 2007;138(suppl):15S-20S.
25. Davies AN, Shorthose K. Parasympathomimetic drugs for the treatment of salivary gland dysfunction due to radiotherapy. Cochrane Database Syst Rev . 2007;(3):CD003782.
26. Petrone D, Condemi JJ, Fife R, et al. A double-blind, randomized, placebo-controlled study of cevimeline in Sjögren’s syndrome patients with xerostomia and keratoconjunctivitis sicca. Arthritis Rheum . 2002;46(3):748-754.
27. Bernardi R, Perin C, Becker FI, et al. Effect of pilocarpine mouthwash on salivary flow. Braz J Med Biol Res . 2002;35(1):105-110.
28. Sasse AD, Clark LG, Sasse EC, et al. Amifostine reduces side effects and improves complete response rate during radiotherapy: results of a meta-analysis. Int J Radiat Oncol Biol Phys . 2006;64(3):784-791.
29. Wasserman TH, Brizel DM, Henke M, et al. Influence of intravenous amifostine on xerostomia, tumor control, and survival after radiotherapy for head-and-neck cancer: 2-year follow-up of a prospective, randomized, phase III trial. Int J Radiat Oncol Biol Phys . 2005;63(4):985-990.
30. Sasse AD, Clark LG, Sasse EC, et al. Amifostine reduces side effects and improves complete response rate during radiotherapy: results of a meta-analysis. Int J Radiat Oncol Biol Phys . 2006;64(3):784-791.
About the Authors
Mahvash Navazesh, DMD, Professor and Chair, Division of Diagnostic Sciences; School of Dentistry, University of Southern California, Los Angeles, California
Satish K.S. Kumar, MDSc, Assistant Professor of Clinical Dentistry, Division of Diagnostic Sciences; School of Dentistry, University of Southern California, Los Angeles, California

Queries for the author may be directed to [email protected] .
Browse Related Categories:

Jul 25, 2014
230 likes | 783 Views
XEROSTOMIA. DEFINITION. Refers to a subject sensation of a dry mouth. Frequently associated with salivary gland hypofunction. A common problem in 25% older adults. CLINICAL FEATURES. in salivary secretion Residual saliva appear foamy or thick and “ropey”
Share Presentation
- syndrome diabetes
- dental disorders symptoms
- fluid intake
- lubricate mouth
- oral disorders xerostomia html
- org complications

Presentation Transcript
DEFINITION • Refers to a subject sensation of a dry mouth. Frequently associated with salivary gland hypofunction. • A common problem in 25% older adults.
CLINICAL FEATURES • in salivary secretion • Residual saliva appear foamy or thick and “ropey” • Examining gloves stick to the oral mucosa • Dorsal tongue often is fissured with atrophy of the filiform papillae • Patient may c/o difficulty in mastication and swallowing and may indicate that food adheres to the oral membranes during eating. • Signs: more prone to dental decay especially at cervical and root caries. Associated more often with radiotherapy aka radiation-induction therapy.
Salivary gland aplasia CAUSES Impaired fluid intake Hemorrhage Vomiting /diarrhea Medication Radiation therapy to head and neck Chemotherapy Sjogren syndrome Diabetes mellitus Diabetes insipidus Sarcoidosis HIV Hep C infection Graft-versus-host-disease Psychogenic disorders mastication Smoking Mouth breathing
MEDICATIONS THAT MAY PRODUCE XEROSTOMIA
Interpretation of findings Xerostomia is diagnosed by symptoms, appearance, and absence of salivary flow when massaging the salivary glands.
Other test Should the presence of xerostomia become unclear:
Management of Xerostomia • Identify the underlying cause • Provide symptomatic treatment where little can be done to alter the underlying cause • It Aims are: • Increase existing saliva flow • Replacing lost secretion • Control dental caries • Control specific measure i.e. infection
Treatment • Drug-related xerostomia: cannot changed to another drug. Schedule to optimize drug effect during the day • Custom-fitted acrylic night guards carrying fluoride gel. • Drugs in liquid should be considered than sublingual osage. • Lubricate mouth and throat with water before swallowing cap. Tab. Or b4 sublingual nitroglycerin • Avoid decongestant and antihistamine
Symptomatic treatment
http://www.merckmanuals.com/professional/dental_disorders/symptoms_of_dental_and_oral_disorders/xerostomia.html http://www.merckmanuals.com/professional/dental_disorders/symptoms_of_dental_and_oral_disorders/xerostomia.html • http://www.oralcancerfoundation.org/complications/xerostomia.php • CONTEMPORARY OPOM, NEVILLE
- More by User

XEROSTOMIA. Presenter: 黃雙玉 2004.09.17. Introduction Symptoms & signs Etiology Diagnosis Management. Introduction. Xerostomia (dry mouth): Defined by Dr. Huchinson,1898. Is not a disease but a symptom caused by many factors. Dr. Ronald
1.21k views • 34 slides

XEROSTOMIA. Defined as the subjective sensation of oral dryness associated with the reduction or absence of saliva output. Xerostomia is a common problem, not a disease. If not recognized and treated, it could have a significant effect on the patient’s quality of life and dental health.
1.19k views • 16 slides

Xerostomia , Xylitol & Xylophones!
Xerostomia , Xylitol & Xylophones!. By: Christian Brennan, Kenia Pereda , and Wendy Li. Learning objectives. Xylitol – What is it? Research on efficacy and MOA Video Xerostomia – What is it? Research on artificial saliva substitute and causes OTC products available Quiz!!!!.
665 views • 21 slides

XEROSTOMIA. Physiology, Etiology, Epidemiology, Pathogenesis, Diagnosis, and Treatment. Reviewed by:. XEROSTOMIA. After viewing this lecture, attendees should be able to:
1.63k views • 41 slides

145 patients with radiation induced xerostomia >18 months
Patients with head and neck cancer treated. with radiotherapy at least 18 months ago. who complain of xerostomia. Randomise. Baseline assessments. Baseline assessments. Group nurse/radiographer specialist. Group acupuncture once a. week for 8 weeks. led educational oral care package.
156 views • 1 slides

Xerostomia. By Emily Wong. Xerostomia :. is defined as dry mouth resulting from reduced or absent of saliva. Importance of saliva:. Lubricates oral cavity Helps chew food Prevents decay Regulate acidity Helps kill bacteria. Causes of xerostomia.
634 views • 9 slides

Xerostomia Therapeutic Pipeline Review, H1 2015
RnRMarketResearch.com adds “Xerostomia Pipeline Review, H1 2015”to its store. The report enhances decision making capabilities and help to create effective counter strategies to gain competitive advantage.
197 views • 6 slides

Xerostomia Global Clinical Trials Review H1 Market Insight, Research, Trend, Size, Growth, Shares and Forecast 2015
ResearchMoz.us has recently released the addition of a new market research report to its repository, titled “Xerostomia Global Clinical Trials Review H1 2015”. Product Synopsis Xerostomia Global Clinical Trials Review, H1, 2015 Summary GlobalData's clinical trial report, Xerostomia Global Clinical Trials Review, H1, 2015" provides an overview of Xerostomia clinical trials scenario. This report provides top line data relating to the clinical trials on Xerostomia . Report includes an overview of trial numbers and their average enrollment in top countries conducted across the globe. The report offers coverage of disease clinical trials by region, country (G7 & E7), phase, trial status, end points status and sponsor type. Report also provides prominent drugs for in-progress trials (based on number of ongoing trials). Global Data Clinical Trial Reports are generated using Global Datas proprietary database - Pharma eTrack Clinical trials database. Clinical trials are collated from 80 different clinical trial registries, conferences, journals, news etc across the globe. Clinical trials database undergoes periodic update by dynamic process. To Browse a Full Report with TOC @ http://www.researchmoz.us/xerostomia-global-clinical-trials-review-h1-2015-report.html The report enhances the decision making capabilities and helps to create an effective counter strategies to gain competitive advantage. *Note: Certain sections in the report may be removed or altered based on the availability and relevance of data for the indicated disease. Scope - The report provides a snapshot of the global clinical trials landscape - Report provides top level data related to the clinical trials by Region, Country (G7 & E7), Trial Status, Trial Phase, Sponsor Type and End point status - The report reviews top companies involved and enlists all trials (Trial title, Phase, and Status) pertaining to the company - The report provides all the unaccomplished trials (Terminated, Suspended and Withdrawn) with reason for unaccomplishment - The Report provides enrollment trends for the past five years - Report provides latest news for the past three months *Note: Certain sections in the report may be removed or altered based on the availability and relevance of data for the indicated disease. To Download Sample Report with TOC @ http://www.researchmoz.us/enquiry.php?type=sample&repid=308795 Reasons to buy - Assists in formulating key business strategies with regards to investment - Helps in identifying prominent locations for conducting clinical trials which saves time and cost - Provides top level analysis of Global Clinical Trials Market which helps in identifying key business opportunities - Supports understanding of trials count and enrollment trends by country in global therapeutics market - Aids in interpreting the success rates of clinical trials by providing a comparative scenario of completed and uncompleted (terminated, suspended or withdrawn) trials - Facilitates clinical trial assessment of the indication on a global, regional and country level *Note: Certain sections in the report may be removed or altered based on the availability and relevance of data for the indicated disease. To Browse all Reports of this Category @ http://www.researchmoz.us/pharmaceutical-market-reports-38.html About ResearchMoz: ResearchMoz is the world’s fastest growing collection of market research reports worldwide. Our database is composed of current market studies from over 100 featured publishers worldwide. Our market research databases integrate statistics with analysis from global, regional, country and company perspectives. ResearchMoz’s service portfolio also includes value-added services such as market research customization, competitive landscaping, and in-depth surveys, delivered by a team of experienced Research Coordinators. Contact Us: Mr. Nachiket State Tower, 90 State Street, Suite 700, Albany NY - 12207 United States Email: [email protected] Blog: http://dynamicmarketresearch.blogspot.com/ Tel: 866-997-4948 (Us-Canada Toll Free) Tel: 1-518-621-2074
195 views • 6 slides

XEROSTOMIA. By : Dr Ebtisam Fetohy 2012.11.21. Introduction Symptoms & signs Etiology Diagnosis Management. Introduction. Xerostomia (dry mouth): Defined by Dr. Huchinson,1898.
411 views • 33 slides

Causes, treatment and prevention of postradiation xerostomia
Causes, treatment and prevention of postradiation xerostomia. By Dr Dimitrios N. Gelis, MD, DDS, ORL Former President of The Greek Society of Otorhinolaryngology-Head and Neck Surgery (2003-2005)
452 views • 44 slides

Global Xerostomia (Dry Mouth) Therapeutics Market Size, Share, Future Prospects and Forecast 2019-2025
Xerostomia (dry mouth) therapeutics market is projected to grow at a considerable CAGR of 7% during the forecast period (2019-2025). As per the American Dental Association, the rate of prevalence of xerostomia in the general population ranges from 0.9% to 64.8%. Severance of xerostomia leads to a critical impact on the patientu2019s health and quality life as it causes oral discomfort to the patient. The rise in the prevalence of Sjogrenu2019s syndrome along with an increase in the consumption of medications is a major factor to drive the growth of the global xerostomia therapeutics market.
58 views • 5 slides

Global Xerostomia (Dry Mouth) Therapeutics Market Size, Competitive Analysis, Share, Forecast- 2019-2025
48 views • 4 slides

Xerostomia Therapeutics Market Strategies and Forecasts, 2020 to 2026
Xerostomia usually called as dry-mouth ailment which occurs due to missing or decreased saliva. Generally, xerostomia is not considered as a disease, yet it is a problem which occurs due to numerous clinical scenarios such as adverse effects of radioactivity on head and also neck usually due to radiation treatment and negative effects of a variety of drugs and it might or might not be always related to the reduced functionality of salivary glands.
80 views • 7 slides
IMAGES
VIDEO
COMMENTS
This page presents a summary of information on xerostomia (the subjective sensation of dry mouth), which is a common complaint among dental patients, particularly older individuals. This page also features a report from the ADA Council on Scientific Affairs on the clinical characteristics and management of xerostomia.
8. Xerostomia affects millions of patients throughout the world. The results of clinical studies suggest that this problem affects mostly menopausal women and individuals above 65 years of age. Etiology There are three most common causes: Sjögren's syndrome (SS), medication and radiotherapy to the head and neck. 9.
Xerostomia. This document discusses xerostomia (dry mouth) and its diagnosis and management in elderly patients. Key points include: - Xerostomia affects 17-29% of populations and is more prevalent in women. It can significantly reduce quality of life. - Saliva plays important roles like maintaining oral health, swallowing, speaking and digestion.
Xerostomia- Dryness of mouth. Sep 25, 2015 • Download as PPTX, PDF •. 83 likes • 16,787 views. Satyaki Verma. Xerostomia is the diesease in which their is absence of saliva in mouth. The slide inlcudes all the helpful subjects about the topic. graphical representation for ease of understanding. Read more. 1 of 29.
Xerostomia refers to the sensation of oral dryness, which can result from diminished saliva production.[1] But, patients may report dry mouth even in the absence of a measurable decrease in saliva quantity.[1] A lack of normal salivary flow may lead to complaints of mouth dryness, oral burning, swallowing difficulty, and loss or decreased taste.[2]
"Explore the world of xerostomia, commonly known as dry mouth, in this comprehensive lecture. Delve into its causes, clinical presentation, and differentials, while discovering effective ...
Presentation Transcript. XEROSTOMIA After viewing this lecture, attendees should be able to: • describe the oral anatomy and physiology related to salivary function as well as the role of saliva in the oral cavity. • discuss the etiology and epidemiology of xerostomia. • relate treatment options for xerostomia.
Xerostomia, also known as dry mouth, can be a consequence of decreased saliva production or flow but may also arise in the absence of a measurable decrease in saliva quantity or flow. Saliva lubricates and cleans the oral cavity, including the oral mucosa. It aids in enhancing an individual's ability to taste and makes it easier to chew and ...
Xerostomia is dry mouth caused by reduced or absent flow of saliva. This condition can result in discomfort, interfere with speech and swallowing, make wearing dentures difficult, cause halitosis, and impair oral hygiene by causing a decrease in oral pH and an increase in bacterial growth. Long-standing xerostomia can result in severe tooth ...
XEROSTOMIA After viewing this lecture, attendees should be able to: describe the oral anatomy and physiology related to salivary function as well as the role of saliva in the oral cavity. discuss the etiology and epidemiology of xerostomia. relate treatment options for xerostomia.
Diagnosis of xerostomia and salivary gland hypofunction is dependent upon a careful and detailed history and thorough oral examination. There exist many options for treatment and symptom management: salivary stimulants, topical agents, saliva substitutes, and systemic sialogogues. The aim of this review is to investigate the current state of ...
The purpose of this systematic review-based guideline is to provide evidence-based recommendations for the prevention and management of salivary gland hypofunction and/or xerostomia induced by nonsurgical cancer therapies including all types of radiation regimens (e.g., head and neck radiation therapy, radioactive iodine, total body irradiation ...
XEROSTOMIA. Presenter: 黃雙玉 2004.09.17. Introduction Symptoms & signs Etiology Diagnosis Management. Introduction. Xerostomia (dry mouth): Defined by Dr. Huchinson,1898. Is not a disease but a symptom caused by many factors. Dr. Ronald
Xerostomia is defined as the complaint of oral dryness. It is a condition that primarily affects older adults and can have a significant negative effect on one's quality of life. Patients with xerostomia often do not have objective signs of hyposalivation. The underlying etiology of xerostomia includes a variety of systemic diseases and local factors. Our aim is to provide a comprehensive ...
Xerostomia, also known as "dry mouth," is a common but frequently overlooked condition that is typically associated with salivary gland hypofunction, which is the objective measurement of reduced salivary flow. Patients with dry mouth exhibit symptoms of variable severity that are commonly attributed to medication use, chronic disease and medical treatment, such as radiotherapy to the head ...
Clinicians may encounter symptoms of xerostomia, commonly called "dry mouth," among patients who take medications, have certain connective tissue or immunological disorders or have been treated with radiation therapy. When xerostomia is the result of a reduction in salivary flow, significant oral complications can occur.
Xerostomia is a common complaint of nearly half of the elderly population and about one-fifth of younger adults. It causes several signs and symptoms, and compromise oral functions and health-related quality-of-life. Multiple reasons are proposed to describe ...
Presentation Transcript. XEROSTOMIA By : Dr Ebtisam Fetohy 2012.11.21. Introduction • Symptoms & signs • Etiology • Diagnosis • Management. Introduction Xerostomia (dry mouth): • Defined by Dr. Huchinson,1898. • Is not a disease but a symptom caused by many factors. Dr.
This article summarizes the common causes, clinical presentation, and complications of xerostomia and salivary gland hypofunction in the geriatric population and discusses the various management options.
XEROSTOMIA. Defined as the subjective sensation of oral dryness associated with the reduction or absence of saliva output. Xerostomia is a common problem, not a disease. If not recognized and treated, it could have a significant effect on the patient's quality of life and dental health.
XEROSTOMIA. DEFINITION. Refers to a subject sensation of a dry mouth. Frequently associated with salivary gland hypofunction. A common problem in 25% older adults. CLINICAL FEATURES. in salivary secretion Residual saliva appear foamy or thick and "ropey". Download Presentation. syndrome diabetes. dental disorders symptoms.