
Community Blog
Keep up-to-date on postgraduate related issues with our quick reads written by students, postdocs, professors and industry leaders.
Types of Research – Explained with Examples
- By DiscoverPhDs
- October 2, 2020

Types of Research
Research is about using established methods to investigate a problem or question in detail with the aim of generating new knowledge about it.
It is a vital tool for scientific advancement because it allows researchers to prove or refute hypotheses based on clearly defined parameters, environments and assumptions. Due to this, it enables us to confidently contribute to knowledge as it allows research to be verified and replicated.
Knowing the types of research and what each of them focuses on will allow you to better plan your project, utilises the most appropriate methodologies and techniques and better communicate your findings to other researchers and supervisors.
Classification of Types of Research
There are various types of research that are classified according to their objective, depth of study, analysed data, time required to study the phenomenon and other factors. It’s important to note that a research project will not be limited to one type of research, but will likely use several.
According to its Purpose
Theoretical research.
Theoretical research, also referred to as pure or basic research, focuses on generating knowledge , regardless of its practical application. Here, data collection is used to generate new general concepts for a better understanding of a particular field or to answer a theoretical research question.
Results of this kind are usually oriented towards the formulation of theories and are usually based on documentary analysis, the development of mathematical formulas and the reflection of high-level researchers.
Applied Research
Here, the goal is to find strategies that can be used to address a specific research problem. Applied research draws on theory to generate practical scientific knowledge, and its use is very common in STEM fields such as engineering, computer science and medicine.
This type of research is subdivided into two types:
- Technological applied research : looks towards improving efficiency in a particular productive sector through the improvement of processes or machinery related to said productive processes.
- Scientific applied research : has predictive purposes. Through this type of research design, we can measure certain variables to predict behaviours useful to the goods and services sector, such as consumption patterns and viability of commercial projects.

According to your Depth of Scope
Exploratory research.
Exploratory research is used for the preliminary investigation of a subject that is not yet well understood or sufficiently researched. It serves to establish a frame of reference and a hypothesis from which an in-depth study can be developed that will enable conclusive results to be generated.
Because exploratory research is based on the study of little-studied phenomena, it relies less on theory and more on the collection of data to identify patterns that explain these phenomena.
Descriptive Research
The primary objective of descriptive research is to define the characteristics of a particular phenomenon without necessarily investigating the causes that produce it.
In this type of research, the researcher must take particular care not to intervene in the observed object or phenomenon, as its behaviour may change if an external factor is involved.
Explanatory Research
Explanatory research is the most common type of research method and is responsible for establishing cause-and-effect relationships that allow generalisations to be extended to similar realities. It is closely related to descriptive research, although it provides additional information about the observed object and its interactions with the environment.
Correlational Research
The purpose of this type of scientific research is to identify the relationship between two or more variables. A correlational study aims to determine whether a variable changes, how much the other elements of the observed system change.
According to the Type of Data Used
Qualitative research.
Qualitative methods are often used in the social sciences to collect, compare and interpret information, has a linguistic-semiotic basis and is used in techniques such as discourse analysis, interviews, surveys, records and participant observations.
In order to use statistical methods to validate their results, the observations collected must be evaluated numerically. Qualitative research, however, tends to be subjective, since not all data can be fully controlled. Therefore, this type of research design is better suited to extracting meaning from an event or phenomenon (the ‘why’) than its cause (the ‘how’).
Quantitative Research
Quantitative research study delves into a phenomena through quantitative data collection and using mathematical, statistical and computer-aided tools to measure them . This allows generalised conclusions to be projected over time.

According to the Degree of Manipulation of Variables
Experimental research.
It is about designing or replicating a phenomenon whose variables are manipulated under strictly controlled conditions in order to identify or discover its effect on another independent variable or object. The phenomenon to be studied is measured through study and control groups, and according to the guidelines of the scientific method.
Non-Experimental Research
Also known as an observational study, it focuses on the analysis of a phenomenon in its natural context. As such, the researcher does not intervene directly, but limits their involvement to measuring the variables required for the study. Due to its observational nature, it is often used in descriptive research.
Quasi-Experimental Research
It controls only some variables of the phenomenon under investigation and is therefore not entirely experimental. In this case, the study and the focus group cannot be randomly selected, but are chosen from existing groups or populations . This is to ensure the collected data is relevant and that the knowledge, perspectives and opinions of the population can be incorporated into the study.
According to the Type of Inference
Deductive investigation.
In this type of research, reality is explained by general laws that point to certain conclusions; conclusions are expected to be part of the premise of the research problem and considered correct if the premise is valid and the inductive method is applied correctly.
Inductive Research
In this type of research, knowledge is generated from an observation to achieve a generalisation. It is based on the collection of specific data to develop new theories.
Hypothetical-Deductive Investigation
It is based on observing reality to make a hypothesis, then use deduction to obtain a conclusion and finally verify or reject it through experience.

According to the Time in Which it is Carried Out
Longitudinal study (also referred to as diachronic research).
It is the monitoring of the same event, individual or group over a defined period of time. It aims to track changes in a number of variables and see how they evolve over time. It is often used in medical, psychological and social areas .
Cross-Sectional Study (also referred to as Synchronous Research)
Cross-sectional research design is used to observe phenomena, an individual or a group of research subjects at a given time.
According to The Sources of Information
Primary research.
This fundamental research type is defined by the fact that the data is collected directly from the source, that is, it consists of primary, first-hand information.
Secondary research
Unlike primary research, secondary research is developed with information from secondary sources, which are generally based on scientific literature and other documents compiled by another researcher.

According to How the Data is Obtained
Documentary (cabinet).
Documentary research, or secondary sources, is based on a systematic review of existing sources of information on a particular subject. This type of scientific research is commonly used when undertaking literature reviews or producing a case study.
Field research study involves the direct collection of information at the location where the observed phenomenon occurs.
From Laboratory
Laboratory research is carried out in a controlled environment in order to isolate a dependent variable and establish its relationship with other variables through scientific methods.
Mixed-Method: Documentary, Field and/or Laboratory
Mixed research methodologies combine results from both secondary (documentary) sources and primary sources through field or laboratory research.

Learn about defining your workspace, having a list of daily tasks and using technology to stay connected, all whilst working from home as a research student.

Thinking about applying to a PhD? Then don’t miss out on these 4 tips on how to best prepare your application.

The unit of analysis refers to the main parameter that you’re investigating in your research project or study.
Join thousands of other students and stay up to date with the latest PhD programmes, funding opportunities and advice.

Browse PhDs Now

Self-plagiarism is when you try and pass off work that you’ve previously done as something that is completely new.

Hannah is a 1st year PhD student at Cardiff Metropolitan University. The aim of her research is to clarify what strategies are the most effective in supporting young people with dyslexia.

Kyle’s in the first year of his PhD at the University of Texas in Austin. His research interests are in the development of algorithms for advanced mobility for legged robotics and computer vision for exploration of extreme environments.
Join Thousands of Students
Qualitative vs Quantitative Research Methods & Data Analysis
Saul Mcleod, PhD
Editor-in-Chief for Simply Psychology
BSc (Hons) Psychology, MRes, PhD, University of Manchester
Saul Mcleod, PhD., is a qualified psychology teacher with over 18 years of experience in further and higher education. He has been published in peer-reviewed journals, including the Journal of Clinical Psychology.
Learn about our Editorial Process
Olivia Guy-Evans, MSc
Associate Editor for Simply Psychology
BSc (Hons) Psychology, MSc Psychology of Education
Olivia Guy-Evans is a writer and associate editor for Simply Psychology. She has previously worked in healthcare and educational sectors.
On This Page:
What is the difference between quantitative and qualitative?
The main difference between quantitative and qualitative research is the type of data they collect and analyze.
Quantitative research collects numerical data and analyzes it using statistical methods. The aim is to produce objective, empirical data that can be measured and expressed in numerical terms. Quantitative research is often used to test hypotheses, identify patterns, and make predictions.
Qualitative research , on the other hand, collects non-numerical data such as words, images, and sounds. The focus is on exploring subjective experiences, opinions, and attitudes, often through observation and interviews.
Qualitative research aims to produce rich and detailed descriptions of the phenomenon being studied, and to uncover new insights and meanings.
Quantitative data is information about quantities, and therefore numbers, and qualitative data is descriptive, and regards phenomenon which can be observed but not measured, such as language.
What Is Qualitative Research?
Qualitative research is the process of collecting, analyzing, and interpreting non-numerical data, such as language. Qualitative research can be used to understand how an individual subjectively perceives and gives meaning to their social reality.
Qualitative data is non-numerical data, such as text, video, photographs, or audio recordings. This type of data can be collected using diary accounts or in-depth interviews and analyzed using grounded theory or thematic analysis.
Qualitative research is multimethod in focus, involving an interpretive, naturalistic approach to its subject matter. This means that qualitative researchers study things in their natural settings, attempting to make sense of, or interpret, phenomena in terms of the meanings people bring to them. Denzin and Lincoln (1994, p. 2)
Interest in qualitative data came about as the result of the dissatisfaction of some psychologists (e.g., Carl Rogers) with the scientific study of psychologists such as behaviorists (e.g., Skinner ).
Since psychologists study people, the traditional approach to science is not seen as an appropriate way of carrying out research since it fails to capture the totality of human experience and the essence of being human. Exploring participants’ experiences is known as a phenomenological approach (re: Humanism ).
Qualitative research is primarily concerned with meaning, subjectivity, and lived experience. The goal is to understand the quality and texture of people’s experiences, how they make sense of them, and the implications for their lives.
Qualitative research aims to understand the social reality of individuals, groups, and cultures as nearly as possible as participants feel or live it. Thus, people and groups are studied in their natural setting.
Some examples of qualitative research questions are provided, such as what an experience feels like, how people talk about something, how they make sense of an experience, and how events unfold for people.
Research following a qualitative approach is exploratory and seeks to explain ‘how’ and ‘why’ a particular phenomenon, or behavior, operates as it does in a particular context. It can be used to generate hypotheses and theories from the data.
Qualitative Methods
There are different types of qualitative research methods, including diary accounts, in-depth interviews , documents, focus groups , case study research , and ethnography.
The results of qualitative methods provide a deep understanding of how people perceive their social realities and in consequence, how they act within the social world.
The researcher has several methods for collecting empirical materials, ranging from the interview to direct observation, to the analysis of artifacts, documents, and cultural records, to the use of visual materials or personal experience. Denzin and Lincoln (1994, p. 14)
Here are some examples of qualitative data:
Interview transcripts : Verbatim records of what participants said during an interview or focus group. They allow researchers to identify common themes and patterns, and draw conclusions based on the data. Interview transcripts can also be useful in providing direct quotes and examples to support research findings.
Observations : The researcher typically takes detailed notes on what they observe, including any contextual information, nonverbal cues, or other relevant details. The resulting observational data can be analyzed to gain insights into social phenomena, such as human behavior, social interactions, and cultural practices.
Unstructured interviews : generate qualitative data through the use of open questions. This allows the respondent to talk in some depth, choosing their own words. This helps the researcher develop a real sense of a person’s understanding of a situation.
Diaries or journals : Written accounts of personal experiences or reflections.
Notice that qualitative data could be much more than just words or text. Photographs, videos, sound recordings, and so on, can be considered qualitative data. Visual data can be used to understand behaviors, environments, and social interactions.
Qualitative Data Analysis
Qualitative research is endlessly creative and interpretive. The researcher does not just leave the field with mountains of empirical data and then easily write up his or her findings.
Qualitative interpretations are constructed, and various techniques can be used to make sense of the data, such as content analysis, grounded theory (Glaser & Strauss, 1967), thematic analysis (Braun & Clarke, 2006), or discourse analysis.
For example, thematic analysis is a qualitative approach that involves identifying implicit or explicit ideas within the data. Themes will often emerge once the data has been coded .

Key Features
- Events can be understood adequately only if they are seen in context. Therefore, a qualitative researcher immerses her/himself in the field, in natural surroundings. The contexts of inquiry are not contrived; they are natural. Nothing is predefined or taken for granted.
- Qualitative researchers want those who are studied to speak for themselves, to provide their perspectives in words and other actions. Therefore, qualitative research is an interactive process in which the persons studied teach the researcher about their lives.
- The qualitative researcher is an integral part of the data; without the active participation of the researcher, no data exists.
- The study’s design evolves during the research and can be adjusted or changed as it progresses. For the qualitative researcher, there is no single reality. It is subjective and exists only in reference to the observer.
- The theory is data-driven and emerges as part of the research process, evolving from the data as they are collected.
Limitations of Qualitative Research
- Because of the time and costs involved, qualitative designs do not generally draw samples from large-scale data sets.
- The problem of adequate validity or reliability is a major criticism. Because of the subjective nature of qualitative data and its origin in single contexts, it is difficult to apply conventional standards of reliability and validity. For example, because of the central role played by the researcher in the generation of data, it is not possible to replicate qualitative studies.
- Also, contexts, situations, events, conditions, and interactions cannot be replicated to any extent, nor can generalizations be made to a wider context than the one studied with confidence.
- The time required for data collection, analysis, and interpretation is lengthy. Analysis of qualitative data is difficult, and expert knowledge of an area is necessary to interpret qualitative data. Great care must be taken when doing so, for example, looking for mental illness symptoms.
Advantages of Qualitative Research
- Because of close researcher involvement, the researcher gains an insider’s view of the field. This allows the researcher to find issues that are often missed (such as subtleties and complexities) by the scientific, more positivistic inquiries.
- Qualitative descriptions can be important in suggesting possible relationships, causes, effects, and dynamic processes.
- Qualitative analysis allows for ambiguities/contradictions in the data, which reflect social reality (Denscombe, 2010).
- Qualitative research uses a descriptive, narrative style; this research might be of particular benefit to the practitioner as she or he could turn to qualitative reports to examine forms of knowledge that might otherwise be unavailable, thereby gaining new insight.
What Is Quantitative Research?
Quantitative research involves the process of objectively collecting and analyzing numerical data to describe, predict, or control variables of interest.
The goals of quantitative research are to test causal relationships between variables , make predictions, and generalize results to wider populations.
Quantitative researchers aim to establish general laws of behavior and phenomenon across different settings/contexts. Research is used to test a theory and ultimately support or reject it.
Quantitative Methods
Experiments typically yield quantitative data, as they are concerned with measuring things. However, other research methods, such as controlled observations and questionnaires , can produce both quantitative information.
For example, a rating scale or closed questions on a questionnaire would generate quantitative data as these produce either numerical data or data that can be put into categories (e.g., “yes,” “no” answers).
Experimental methods limit how research participants react to and express appropriate social behavior.
Findings are, therefore, likely to be context-bound and simply a reflection of the assumptions that the researcher brings to the investigation.
There are numerous examples of quantitative data in psychological research, including mental health. Here are a few examples:
Another example is the Experience in Close Relationships Scale (ECR), a self-report questionnaire widely used to assess adult attachment styles .
The ECR provides quantitative data that can be used to assess attachment styles and predict relationship outcomes.
Neuroimaging data : Neuroimaging techniques, such as MRI and fMRI, provide quantitative data on brain structure and function.
This data can be analyzed to identify brain regions involved in specific mental processes or disorders.
For example, the Beck Depression Inventory (BDI) is a clinician-administered questionnaire widely used to assess the severity of depressive symptoms in individuals.
The BDI consists of 21 questions, each scored on a scale of 0 to 3, with higher scores indicating more severe depressive symptoms.
Quantitative Data Analysis
Statistics help us turn quantitative data into useful information to help with decision-making. We can use statistics to summarize our data, describing patterns, relationships, and connections. Statistics can be descriptive or inferential.
Descriptive statistics help us to summarize our data. In contrast, inferential statistics are used to identify statistically significant differences between groups of data (such as intervention and control groups in a randomized control study).
- Quantitative researchers try to control extraneous variables by conducting their studies in the lab.
- The research aims for objectivity (i.e., without bias) and is separated from the data.
- The design of the study is determined before it begins.
- For the quantitative researcher, the reality is objective, exists separately from the researcher, and can be seen by anyone.
- Research is used to test a theory and ultimately support or reject it.
Limitations of Quantitative Research
- Context: Quantitative experiments do not take place in natural settings. In addition, they do not allow participants to explain their choices or the meaning of the questions they may have for those participants (Carr, 1994).
- Researcher expertise: Poor knowledge of the application of statistical analysis may negatively affect analysis and subsequent interpretation (Black, 1999).
- Variability of data quantity: Large sample sizes are needed for more accurate analysis. Small-scale quantitative studies may be less reliable because of the low quantity of data (Denscombe, 2010). This also affects the ability to generalize study findings to wider populations.
- Confirmation bias: The researcher might miss observing phenomena because of focus on theory or hypothesis testing rather than on the theory of hypothesis generation.
Advantages of Quantitative Research
- Scientific objectivity: Quantitative data can be interpreted with statistical analysis, and since statistics are based on the principles of mathematics, the quantitative approach is viewed as scientifically objective and rational (Carr, 1994; Denscombe, 2010).
- Useful for testing and validating already constructed theories.
- Rapid analysis: Sophisticated software removes much of the need for prolonged data analysis, especially with large volumes of data involved (Antonius, 2003).
- Replication: Quantitative data is based on measured values and can be checked by others because numerical data is less open to ambiguities of interpretation.
- Hypotheses can also be tested because of statistical analysis (Antonius, 2003).
Antonius, R. (2003). Interpreting quantitative data with SPSS . Sage.
Black, T. R. (1999). Doing quantitative research in the social sciences: An integrated approach to research design, measurement and statistics . Sage.
Braun, V. & Clarke, V. (2006). Using thematic analysis in psychology . Qualitative Research in Psychology , 3, 77–101.
Carr, L. T. (1994). The strengths and weaknesses of quantitative and qualitative research : what method for nursing? Journal of advanced nursing, 20(4) , 716-721.
Denscombe, M. (2010). The Good Research Guide: for small-scale social research. McGraw Hill.
Denzin, N., & Lincoln. Y. (1994). Handbook of Qualitative Research. Thousand Oaks, CA, US: Sage Publications Inc.
Glaser, B. G., Strauss, A. L., & Strutzel, E. (1968). The discovery of grounded theory; strategies for qualitative research. Nursing research, 17(4) , 364.
Minichiello, V. (1990). In-Depth Interviewing: Researching People. Longman Cheshire.
Punch, K. (1998). Introduction to Social Research: Quantitative and Qualitative Approaches. London: Sage
Further Information
- Designing qualitative research
- Methods of data collection and analysis
- Introduction to quantitative and qualitative research
- Checklists for improving rigour in qualitative research: a case of the tail wagging the dog?
- Qualitative research in health care: Analysing qualitative data
- Qualitative data analysis: the framework approach
- Using the framework method for the analysis of
- Qualitative data in multi-disciplinary health research
- Content Analysis
- Grounded Theory
- Thematic Analysis
Related Articles

Research Methodology
Qualitative Data Coding

What Is a Focus Group?

Cross-Cultural Research Methodology In Psychology

What Is Internal Validity In Research?

Research Methodology , Statistics
What Is Face Validity In Research? Importance & How To Measure

Criterion Validity: Definition & Examples

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Turk J Anaesthesiol Reanim
- v.44(4); 2016 Aug
What is Scientific Research and How Can it be Done?
Scientific researches are studies that should be systematically planned before performing them. In this review, classification and description of scientific studies, planning stage randomisation and bias are explained.
Research conducted for the purpose of contributing towards science by the systematic collection, interpretation and evaluation of data and that, too, in a planned manner is called scientific research: a researcher is the one who conducts this research. The results obtained from a small group through scientific studies are socialised, and new information is revealed with respect to diagnosis, treatment and reliability of applications. The purpose of this review is to provide information about the definition, classification and methodology of scientific research.
Before beginning the scientific research, the researcher should determine the subject, do planning and specify the methodology. In the Declaration of Helsinki, it is stated that ‘the primary purpose of medical researches on volunteers is to understand the reasons, development and effects of diseases and develop protective, diagnostic and therapeutic interventions (method, operation and therapies). Even the best proven interventions should be evaluated continuously by investigations with regard to reliability, effectiveness, efficiency, accessibility and quality’ ( 1 ).
The questions, methods of response to questions and difficulties in scientific research may vary, but the design and structure are generally the same ( 2 ).
Classification of Scientific Research
Scientific research can be classified in several ways. Classification can be made according to the data collection techniques based on causality, relationship with time and the medium through which they are applied.
- Observational
- Experimental
- Descriptive
- Retrospective
- Prospective
- Cross-sectional
- Social descriptive research ( 3 )
Another method is to classify the research according to its descriptive or analytical features. This review is written according to this classification method.
I. Descriptive research
- Case series
- Surveillance studies
II. Analytical research
- Observational studies: cohort, case control and cross- sectional research
- Interventional research: quasi-experimental and clinical research
- Case Report: it is the most common type of descriptive study. It is the examination of a single case having a different quality in the society, e.g. conducting general anaesthesia in a pregnant patient with mucopolysaccharidosis.
- Case Series: it is the description of repetitive cases having common features. For instance; case series involving interscapular pain related to neuraxial labour analgesia. Interestingly, malignant hyperthermia cases are not accepted as case series since they are rarely seen during historical development.
- Surveillance Studies: these are the results obtained from the databases that follow and record a health problem for a certain time, e.g. the surveillance of cross-infections during anaesthesia in the intensive care unit.
Moreover, some studies may be experimental. After the researcher intervenes, the researcher waits for the result, observes and obtains data. Experimental studies are, more often, in the form of clinical trials or laboratory animal trials ( 2 ).
Analytical observational research can be classified as cohort, case-control and cross-sectional studies.
Firstly, the participants are controlled with regard to the disease under investigation. Patients are excluded from the study. Healthy participants are evaluated with regard to the exposure to the effect. Then, the group (cohort) is followed-up for a sufficient period of time with respect to the occurrence of disease, and the progress of disease is studied. The risk of the healthy participants getting sick is considered an incident. In cohort studies, the risk of disease between the groups exposed and not exposed to the effect is calculated and rated. This rate is called relative risk. Relative risk indicates the strength of exposure to the effect on the disease.
Cohort research may be observational and experimental. The follow-up of patients prospectively is called a prospective cohort study . The results are obtained after the research starts. The researcher’s following-up of cohort subjects from a certain point towards the past is called a retrospective cohort study . Prospective cohort studies are more valuable than retrospective cohort studies: this is because in the former, the researcher observes and records the data. The researcher plans the study before the research and determines what data will be used. On the other hand, in retrospective studies, the research is made on recorded data: no new data can be added.
In fact, retrospective and prospective studies are not observational. They determine the relationship between the date on which the researcher has begun the study and the disease development period. The most critical disadvantage of this type of research is that if the follow-up period is long, participants may leave the study at their own behest or due to physical conditions. Cohort studies that begin after exposure and before disease development are called ambidirectional studies . Public healthcare studies generally fall within this group, e.g. lung cancer development in smokers.
- Case-Control Studies: these studies are retrospective cohort studies. They examine the cause and effect relationship from the effect to the cause. The detection or determination of data depends on the information recorded in the past. The researcher has no control over the data ( 2 ).
Cross-sectional studies are advantageous since they can be concluded relatively quickly. It may be difficult to obtain a reliable result from such studies for rare diseases ( 2 ).
Cross-sectional studies are characterised by timing. In such studies, the exposure and result are simultaneously evaluated. While cross-sectional studies are restrictedly used in studies involving anaesthesia (since the process of exposure is limited), they can be used in studies conducted in intensive care units.
- Quasi-Experimental Research: they are conducted in cases in which a quick result is requested and the participants or research areas cannot be randomised, e.g. giving hand-wash training and comparing the frequency of nosocomial infections before and after hand wash.
- Clinical Research: they are prospective studies carried out with a control group for the purpose of comparing the effect and value of an intervention in a clinical case. Clinical study and research have the same meaning. Drugs, invasive interventions, medical devices and operations, diets, physical therapy and diagnostic tools are relevant in this context ( 6 ).
Clinical studies are conducted by a responsible researcher, generally a physician. In the research team, there may be other healthcare staff besides physicians. Clinical studies may be financed by healthcare institutes, drug companies, academic medical centres, volunteer groups, physicians, healthcare service providers and other individuals. They may be conducted in several places including hospitals, universities, physicians’ offices and community clinics based on the researcher’s requirements. The participants are made aware of the duration of the study before their inclusion. Clinical studies should include the evaluation of recommendations (drug, device and surgical) for the treatment of a disease, syndrome or a comparison of one or more applications; finding different ways for recognition of a disease or case and prevention of their recurrence ( 7 ).
Clinical Research
In this review, clinical research is explained in more detail since it is the most valuable study in scientific research.
Clinical research starts with forming a hypothesis. A hypothesis can be defined as a claim put forward about the value of a population parameter based on sampling. There are two types of hypotheses in statistics.
- H 0 hypothesis is called a control or null hypothesis. It is the hypothesis put forward in research, which implies that there is no difference between the groups under consideration. If this hypothesis is rejected at the end of the study, it indicates that a difference exists between the two treatments under consideration.
- H 1 hypothesis is called an alternative hypothesis. It is hypothesised against a null hypothesis, which implies that a difference exists between the groups under consideration. For example, consider the following hypothesis: drug A has an analgesic effect. Control or null hypothesis (H 0 ): there is no difference between drug A and placebo with regard to the analgesic effect. The alternative hypothesis (H 1 ) is applicable if a difference exists between drug A and placebo with regard to the analgesic effect.
The planning phase comes after the determination of a hypothesis. A clinical research plan is called a protocol . In a protocol, the reasons for research, number and qualities of participants, tests to be applied, study duration and what information to be gathered from the participants should be found and conformity criteria should be developed.
The selection of participant groups to be included in the study is important. Inclusion and exclusion criteria of the study for the participants should be determined. Inclusion criteria should be defined in the form of demographic characteristics (age, gender, etc.) of the participant group and the exclusion criteria as the diseases that may influence the study, age ranges, cases involving pregnancy and lactation, continuously used drugs and participants’ cooperation.
The next stage is methodology. Methodology can be grouped under subheadings, namely, the calculation of number of subjects, blinding (masking), randomisation, selection of operation to be applied, use of placebo and criteria for stopping and changing the treatment.
I. Calculation of the Number of Subjects
The entire source from which the data are obtained is called a universe or population . A small group selected from a certain universe based on certain rules and which is accepted to highly represent the universe from which it is selected is called a sample and the characteristics of the population from which the data are collected are called variables. If data is collected from the entire population, such an instance is called a parameter . Conducting a study on the sample rather than the entire population is easier and less costly. Many factors influence the determination of the sample size. Firstly, the type of variable should be determined. Variables are classified as categorical (qualitative, non-numerical) or numerical (quantitative). Individuals in categorical variables are classified according to their characteristics. Categorical variables are indicated as nominal and ordinal (ordered). In nominal variables, the application of a category depends on the researcher’s preference. For instance, a female participant can be considered first and then the male participant, or vice versa. An ordinal (ordered) variable is ordered from small to large or vice versa (e.g. ordering obese patients based on their weights-from the lightest to the heaviest or vice versa). A categorical variable may have more than one characteristic: such variables are called binary or dichotomous (e.g. a participant may be both female and obese).
If the variable has numerical (quantitative) characteristics and these characteristics cannot be categorised, then it is called a numerical variable. Numerical variables are either discrete or continuous. For example, the number of operations with spinal anaesthesia represents a discrete variable. The haemoglobin value or height represents a continuous variable.
Statistical analyses that need to be employed depend on the type of variable. The determination of variables is necessary for selecting the statistical method as well as software in SPSS. While categorical variables are presented as numbers and percentages, numerical variables are represented using measures such as mean and standard deviation. It may be necessary to use mean in categorising some cases such as the following: even though the variable is categorical (qualitative, non-numerical) when Visual Analogue Scale (VAS) is used (since a numerical value is obtained), it is classified as a numerical variable: such variables are averaged.
Clinical research is carried out on the sample and generalised to the population. Accordingly, the number of samples should be correctly determined. Different sample size formulas are used on the basis of the statistical method to be used. When the sample size increases, error probability decreases. The sample size is calculated based on the primary hypothesis. The determination of a sample size before beginning the research specifies the power of the study. Power analysis enables the acquisition of realistic results in the research, and it is used for comparing two or more clinical research methods.
Because of the difference in the formulas used in calculating power analysis and number of samples for clinical research, it facilitates the use of computer programs for making calculations.
It is necessary to know certain parameters in order to calculate the number of samples by power analysis.
- Type-I (α) and type-II (β) error levels
- Difference between groups (d-difference) and effect size (ES)
- Distribution ratio of groups
- Direction of research hypothesis (H1)
a. Type-I (α) and Type-II (β) Error (β) Levels
Two types of errors can be made while accepting or rejecting H 0 hypothesis in a hypothesis test. Type-I error (α) level is the probability of finding a difference at the end of the research when there is no difference between the two applications. In other words, it is the rejection of the hypothesis when H 0 is actually correct and it is known as α error or p value. For instance, when the size is determined, type-I error level is accepted as 0.05 or 0.01.
Another error that can be made during a hypothesis test is a type-II error. It is the acceptance of a wrongly hypothesised H 0 hypothesis. In fact, it is the probability of failing to find a difference when there is a difference between the two applications. The power of a test is the ability of that test to find a difference that actually exists. Therefore, it is related to the type-II error level.
Since the type-II error risk is expressed as β, the power of the test is defined as 1–β. When a type-II error is 0.20, the power of the test is 0.80. Type-I (α) and type-II (β) errors can be intentional. The reason to intentionally make such an error is the necessity to look at the events from the opposite perspective.
b. Difference between Groups and ES
ES is defined as the state in which statistical difference also has clinically significance: ES≥0.5 is desirable. The difference between groups is the absolute difference between the groups compared in clinical research.
c. Allocation Ratio of Groups
The allocation ratio of groups is effective in determining the number of samples. If the number of samples is desired to be determined at the lowest level, the rate should be kept as 1/1.
d. Direction of Hypothesis (H1)
The direction of hypothesis in clinical research may be one-sided or two-sided. While one-sided hypotheses hypothesis test differences in the direction of size, two-sided hypotheses hypothesis test differences without direction. The power of the test in two-sided hypotheses is lower than one-sided hypotheses.
After these four variables are determined, they are entered in the appropriate computer program and the number of samples is calculated. Statistical packaged software programs such as Statistica, NCSS and G-Power may be used for power analysis and calculating the number of samples. When the samples size is calculated, if there is a decrease in α, difference between groups, ES and number of samples, then the standard deviation increases and power decreases. The power in two-sided hypothesis is lower. It is ethically appropriate to consider the determination of sample size, particularly in animal experiments, at the beginning of the study. The phase of the study is also important in the determination of number of subjects to be included in drug studies. Usually, phase-I studies are used to determine the safety profile of a drug or product, and they are generally conducted on a few healthy volunteers. If no unacceptable toxicity is detected during phase-I studies, phase-II studies may be carried out. Phase-II studies are proof-of-concept studies conducted on a larger number (100–500) of volunteer patients. When the effectiveness of the drug or product is evident in phase-II studies, phase-III studies can be initiated. These are randomised, double-blinded, placebo or standard treatment-controlled studies. Volunteer patients are periodically followed-up with respect to the effectiveness and side effects of the drug. It can generally last 1–4 years and is valuable during licensing and releasing the drug to the general market. Then, phase-IV studies begin in which long-term safety is investigated (indication, dose, mode of application, safety, effectiveness, etc.) on thousands of volunteer patients.
II. Blinding (Masking) and Randomisation Methods
When the methodology of clinical research is prepared, precautions should be taken to prevent taking sides. For this reason, techniques such as randomisation and blinding (masking) are used. Comparative studies are the most ideal ones in clinical research.
Blinding Method
A case in which the treatments applied to participants of clinical research should be kept unknown is called the blinding method . If the participant does not know what it receives, it is called a single-blind study; if even the researcher does not know, it is called a double-blind study. When there is a probability of knowing which drug is given in the order of application, when uninformed staff administers the drug, it is called in-house blinding. In case the study drug is known in its pharmaceutical form, a double-dummy blinding test is conducted. Intravenous drug is given to one group and a placebo tablet is given to the comparison group; then, the placebo tablet is given to the group that received the intravenous drug and intravenous drug in addition to placebo tablet is given to the comparison group. In this manner, each group receives both the intravenous and tablet forms of the drug. In case a third party interested in the study is involved and it also does not know about the drug (along with the statistician), it is called third-party blinding.
Randomisation Method
The selection of patients for the study groups should be random. Randomisation methods are used for such selection, which prevent conscious or unconscious manipulations in the selection of patients ( 8 ).
No factor pertaining to the patient should provide preference of one treatment to the other during randomisation. This characteristic is the most important difference separating randomised clinical studies from prospective and synchronous studies with experimental groups. Randomisation strengthens the study design and enables the determination of reliable scientific knowledge ( 2 ).
The easiest method is simple randomisation, e.g. determination of the type of anaesthesia to be administered to a patient by tossing a coin. In this method, when the number of samples is kept high, a balanced distribution is created. When the number of samples is low, there will be an imbalance between the groups. In this case, stratification and blocking have to be added to randomisation. Stratification is the classification of patients one or more times according to prognostic features determined by the researcher and blocking is the selection of a certain number of patients for each stratification process. The number of stratification processes should be determined at the beginning of the study.
As the number of stratification processes increases, performing the study and balancing the groups become difficult. For this reason, stratification characteristics and limitations should be effectively determined at the beginning of the study. It is not mandatory for the stratifications to have equal intervals. Despite all the precautions, an imbalance might occur between the groups before beginning the research. In such circumstances, post-stratification or restandardisation may be conducted according to the prognostic factors.
The main characteristic of applying blinding (masking) and randomisation is the prevention of bias. Therefore, it is worthwhile to comprehensively examine bias at this stage.
Bias and Chicanery
While conducting clinical research, errors can be introduced voluntarily or involuntarily at a number of stages, such as design, population selection, calculating the number of samples, non-compliance with study protocol, data entry and selection of statistical method. Bias is taking sides of individuals in line with their own decisions, views and ideological preferences ( 9 ). In order for an error to lead to bias, it has to be a systematic error. Systematic errors in controlled studies generally cause the results of one group to move in a different direction as compared to the other. It has to be understood that scientific research is generally prone to errors. However, random errors (or, in other words, ‘the luck factor’-in which bias is unintended-do not lead to bias ( 10 ).
Another issue, which is different from bias, is chicanery. It is defined as voluntarily changing the interventions, results and data of patients in an unethical manner or copying data from other studies. Comparatively, bias may not be done consciously.
In case unexpected results or outliers are found while the study is analysed, if possible, such data should be re-included into the study since the complete exclusion of data from a study endangers its reliability. In such a case, evaluation needs to be made with and without outliers. It is insignificant if no difference is found. However, if there is a difference, the results with outliers are re-evaluated. If there is no error, then the outlier is included in the study (as the outlier may be a result). It should be noted that re-evaluation of data in anaesthesiology is not possible.
Statistical evaluation methods should be determined at the design stage so as not to encounter unexpected results in clinical research. The data should be evaluated before the end of the study and without entering into details in research that are time-consuming and involve several samples. This is called an interim analysis . The date of interim analysis should be determined at the beginning of the study. The purpose of making interim analysis is to prevent unnecessary cost and effort since it may be necessary to conclude the research after the interim analysis, e.g. studies in which there is no possibility to validate the hypothesis at the end or the occurrence of different side effects of the drug to be used. The accuracy of the hypothesis and number of samples are compared. Statistical significance levels in interim analysis are very important. If the data level is significant, the hypothesis is validated even if the result turns out to be insignificant after the date of the analysis.
Another important point to be considered is the necessity to conclude the participants’ treatment within the period specified in the study protocol. When the result of the study is achieved earlier and unexpected situations develop, the treatment is concluded earlier. Moreover, the participant may quit the study at its own behest, may die or unpredictable situations (e.g. pregnancy) may develop. The participant can also quit the study whenever it wants, even if the study has not ended ( 7 ).
In case the results of a study are contrary to already known or expected results, the expected quality level of the study suggesting the contradiction may be higher than the studies supporting what is known in that subject. This type of bias is called confirmation bias. The presence of well-known mechanisms and logical inference from them may create problems in the evaluation of data. This is called plausibility bias.
Another type of bias is expectation bias. If a result different from the known results has been achieved and it is against the editor’s will, it can be challenged. Bias may be introduced during the publication of studies, such as publishing only positive results, selection of study results in a way to support a view or prevention of their publication. Some editors may only publish research that extols only the positive results or results that they desire.
Bias may be introduced for advertisement or economic reasons. Economic pressure may be applied on the editor, particularly in the cases of studies involving drugs and new medical devices. This is called commercial bias.
In recent years, before beginning a study, it has been recommended to record it on the Web site www.clinicaltrials.gov for the purpose of facilitating systematic interpretation and analysis in scientific research, informing other researchers, preventing bias, provision of writing in a standard format, enhancing contribution of research results to the general literature and enabling early intervention of an institution for support. This Web site is a service of the US National Institutes of Health.
The last stage in the methodology of clinical studies is the selection of intervention to be conducted. Placebo use assumes an important place in interventions. In Latin, placebo means ‘I will be fine’. In medical literature, it refers to substances that are not curative, do not have active ingredients and have various pharmaceutical forms. Although placebos do not have active drug characteristic, they have shown effective analgesic characteristics, particularly in algology applications; further, its use prevents bias in comparative studies. If a placebo has a positive impact on a participant, it is called the placebo effect ; on the contrary, if it has a negative impact, it is called the nocebo effect . Another type of therapy that can be used in clinical research is sham application. Although a researcher does not cure the patient, the researcher may compare those who receive therapy and undergo sham. It has been seen that sham therapies also exhibit a placebo effect. In particular, sham therapies are used in acupuncture applications ( 11 ). While placebo is a substance, sham is a type of clinical application.
Ethically, the patient has to receive appropriate therapy. For this reason, if its use prevents effective treatment, it causes great problem with regard to patient health and legalities.
Before medical research is conducted with human subjects, predictable risks, drawbacks and benefits must be evaluated for individuals or groups participating in the study. Precautions must be taken for reducing the risk to a minimum level. The risks during the study should be followed, evaluated and recorded by the researcher ( 1 ).
After the methodology for a clinical study is determined, dealing with the ‘Ethics Committee’ forms the next stage. The purpose of the ethics committee is to protect the rights, safety and well-being of volunteers taking part in the clinical research, considering the scientific method and concerns of society. The ethics committee examines the studies presented in time, comprehensively and independently, with regard to ethics and science; in line with the Declaration of Helsinki and following national and international standards concerning ‘Good Clinical Practice’. The method to be followed in the formation of the ethics committee should be developed without any kind of prejudice and to examine the applications with regard to ethics and science within the framework of the ethics committee, Regulation on Clinical Trials and Good Clinical Practice ( www.iku.com ). The necessary documents to be presented to the ethics committee are research protocol, volunteer consent form, budget contract, Declaration of Helsinki, curriculum vitae of researchers, similar or explanatory literature samples, supporting institution approval certificate and patient follow-up form.
Only one sister/brother, mother, father, son/daughter and wife/husband can take charge in the same ethics committee. A rector, vice rector, dean, deputy dean, provincial healthcare director and chief physician cannot be members of the ethics committee.
Members of the ethics committee can work as researchers or coordinators in clinical research. However, during research meetings in which members of the ethics committee are researchers or coordinators, they must leave the session and they cannot sign-off on decisions. If the number of members in the ethics committee for a particular research is so high that it is impossible to take a decision, the clinical research is presented to another ethics committee in the same province. If there is no ethics committee in the same province, an ethics committee in the closest settlement is found.
Thereafter, researchers need to inform the participants using an informed consent form. This form should explain the content of clinical study, potential benefits of the study, alternatives and risks (if any). It should be easy, comprehensible, conforming to spelling rules and written in plain language understandable by the participant.
This form assists the participants in taking a decision regarding participation in the study. It should aim to protect the participants. The participant should be included in the study only after it signs the informed consent form; the participant can quit the study whenever required, even when the study has not ended ( 7 ).
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - C.Ö.Ç., A.D.; Design - C.Ö.Ç.; Supervision - A.D.; Resource - C.Ö.Ç., A.D.; Materials - C.Ö.Ç., A.D.; Analysis and/or Interpretation - C.Ö.Ç., A.D.; Literature Search - C.Ö.Ç.; Writing Manuscript - C.Ö.Ç.; Critical Review - A.D.; Other - C.Ö.Ç., A.D.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
Official websites use .gov
A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS
A lock ( ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
Understanding the Notice of Funding Opportunity (NOFO)
How to Apply
‹ View Table of Contents
Follow the detailed instructions in the Notice of Funding Opportunity (NOFO) and in the application guide carefully. In general, CDC’s NOFOs follow a basic structure outlined below. This structure may change depending on the project and announcement.
General Structure of CDC’s NOFO
Part 1: overview includes information such as:.
- Type of funding mechanism, i.e. grant or cooperative agreement
- Notice of Funding Opportunity (NOFO) title and number
- Important application dates, i.e. Pre-application deadline, application deadline, informational conference call date
- Executive summary
- Expected number of awards
- Funding information (e.g., maximum, minimum amount per award)
- Approximate award date
- Cost-sharing and/or matching requirements
Part 2: Full Text includes information such as:
- Description of funding opportunity (e.g., proposed activities, purpose, resources)
- Award information
- Description of eligible applicant types
- Application and submission information
- Application review information
- Award administration information
- Agency contact information
- Other information
Types of CDC Funding Opportunities
CDC funds research and non-research grants and cooperative agreements.
The major difference between research and non-research lies in the purpose of the activity. The purpose of research is to increase scientific knowledge. The purpose of non-research in public health is to prevent or control disease or injury and improve health, or to improve a public health program or service.
A research grant or cooperative agreement provides funding to support investigatory projects to be performed by specific organizations in their areas of expertise. Research means a “systematic investigation, including research development, testing and evaluation, designed to develop or contribute to generalizable knowledge” (45 CFR 46.102(d)).
A non-research grant or cooperative agreement provides funding to support the agency’s programmatic needs, such as HIV prevention projects and programs for children’s immunization and vaccines. The purpose of the non-research activity is to identify and control a health problem or improve a public health program or service. Intended benefits of the project are primarily or exclusively for the participants (or clients) or the participants’ community; data collected are needed to assess or improve the program or service, the health of the participants or the participants’ community; knowledge that is generated does not extend beyond the scope of the activity; and project activities are not experimental.
For more information, visit CDC’s policy on distinguishing research and non-research grants .
Applying for a Notice of Funding Opportunity (NOFO)
- Eligibility
- Pre-Award Activities for Applicants
- Key Steps of the Application Process
- Tips for Preparing Grant Applications
- › Understanding the Notice of Funding Opportunity (NOFO)
- Find Funding Opportunities
- Understand the Review Process
- Frequently Asked Questions
- Application Resources
Exit Notification / Disclaimer Policy
- The Centers for Disease Control and Prevention (CDC) cannot attest to the accuracy of a non-federal website.
- Linking to a non-federal website does not constitute an endorsement by CDC or any of its employees of the sponsors or the information and products presented on the website.
- You will be subject to the destination website's privacy policy when you follow the link.
- CDC is not responsible for Section 508 compliance (accessibility) on other federal or private website.
Child Care and Early Education Research Connections
Experiments and quasi-experiments.
This page includes an explanation of the types, key components, validity, ethics, and advantages and disadvantages of experimental design.
An experiment is a study in which the researcher manipulates the level of some independent variable and then measures the outcome. Experiments are powerful techniques for evaluating cause-and-effect relationships. Many researchers consider experiments the "gold standard" against which all other research designs should be judged. Experiments are conducted both in the laboratory and in real life situations.
Types of Experimental Design
There are two basic types of research design:
- True experiments
- Quasi-experiments
The purpose of both is to examine the cause of certain phenomena.
True experiments, in which all the important factors that might affect the phenomena of interest are completely controlled, are the preferred design. Often, however, it is not possible or practical to control all the key factors, so it becomes necessary to implement a quasi-experimental research design.
Similarities between true and quasi-experiments:
- Study participants are subjected to some type of treatment or condition
- Some outcome of interest is measured
- The researchers test whether differences in this outcome are related to the treatment
Differences between true experiments and quasi-experiments:
- In a true experiment, participants are randomly assigned to either the treatment or the control group, whereas they are not assigned randomly in a quasi-experiment
- In a quasi-experiment, the control and treatment groups differ not only in terms of the experimental treatment they receive, but also in other, often unknown or unknowable, ways. Thus, the researcher must try to statistically control for as many of these differences as possible
- Because control is lacking in quasi-experiments, there may be several "rival hypotheses" competing with the experimental manipulation as explanations for observed results
Key Components of Experimental Research Design
The manipulation of predictor variables.
In an experiment, the researcher manipulates the factor that is hypothesized to affect the outcome of interest. The factor that is being manipulated is typically referred to as the treatment or intervention. The researcher may manipulate whether research subjects receive a treatment (e.g., antidepressant medicine: yes or no) and the level of treatment (e.g., 50 mg, 75 mg, 100 mg, and 125 mg).
Suppose, for example, a group of researchers was interested in the causes of maternal employment. They might hypothesize that the provision of government-subsidized child care would promote such employment. They could then design an experiment in which some subjects would be provided the option of government-funded child care subsidies and others would not. The researchers might also manipulate the value of the child care subsidies in order to determine if higher subsidy values might result in different levels of maternal employment.
Random Assignment
- Study participants are randomly assigned to different treatment groups
- All participants have the same chance of being in a given condition
- Participants are assigned to either the group that receives the treatment, known as the "experimental group" or "treatment group," or to the group which does not receive the treatment, referred to as the "control group"
- Random assignment neutralizes factors other than the independent and dependent variables, making it possible to directly infer cause and effect
Random Sampling
Traditionally, experimental researchers have used convenience sampling to select study participants. However, as research methods have become more rigorous, and the problems with generalizing from a convenience sample to the larger population have become more apparent, experimental researchers are increasingly turning to random sampling. In experimental policy research studies, participants are often randomly selected from program administrative databases and randomly assigned to the control or treatment groups.
Validity of Results
The two types of validity of experiments are internal and external. It is often difficult to achieve both in social science research experiments.
Internal Validity
- When an experiment is internally valid, we are certain that the independent variable (e.g., child care subsidies) caused the outcome of the study (e.g., maternal employment)
- When subjects are randomly assigned to treatment or control groups, we can assume that the independent variable caused the observed outcomes because the two groups should not have differed from one another at the start of the experiment
- For example, take the child care subsidy example above. Since research subjects were randomly assigned to the treatment (child care subsidies available) and control (no child care subsidies available) groups, the two groups should not have differed at the outset of the study. If, after the intervention, mothers in the treatment group were more likely to be working, we can assume that the availability of child care subsidies promoted maternal employment
One potential threat to internal validity in experiments occurs when participants either drop out of the study or refuse to participate in the study. If particular types of individuals drop out or refuse to participate more often than individuals with other characteristics, this is called differential attrition. For example, suppose an experiment was conducted to assess the effects of a new reading curriculum. If the new curriculum was so tough that many of the slowest readers dropped out of school, the school with the new curriculum would experience an increase in the average reading scores. The reason they experienced an increase in reading scores, however, is because the worst readers left the school, not because the new curriculum improved students' reading skills.
External Validity
- External validity is also of particular concern in social science experiments
- It can be very difficult to generalize experimental results to groups that were not included in the study
- Studies that randomly select participants from the most diverse and representative populations are more likely to have external validity
- The use of random sampling techniques makes it easier to generalize the results of studies to other groups
For example, a research study shows that a new curriculum improved reading comprehension of third-grade children in Iowa. To assess the study's external validity, you would ask whether this new curriculum would also be effective with third graders in New York or with children in other elementary grades.
Glossary terms related to validity:
- internal validity
- external validity
- differential attrition
It is particularly important in experimental research to follow ethical guidelines. Protecting the health and safety of research subjects is imperative. In order to assure subject safety, all researchers should have their project reviewed by the Institutional Review Boards (IRBS). The National Institutes of Health supplies strict guidelines for project approval. Many of these guidelines are based on the Belmont Report (pdf).
The basic ethical principles:
- Respect for persons -- requires that research subjects are not coerced into participating in a study and requires the protection of research subjects who have diminished autonomy
- Beneficence -- requires that experiments do not harm research subjects, and that researchers minimize the risks for subjects while maximizing the benefits for them
- Justice -- requires that all forms of differential treatment among research subjects be justified
Advantages and Disadvantages of Experimental Design
The environment in which the research takes place can often be carefully controlled. Consequently, it is easier to estimate the true effect of the variable of interest on the outcome of interest.
Disadvantages
It is often difficult to assure the external validity of the experiment, due to the frequently nonrandom selection processes and the artificial nature of the experimental context.

Performing Academic Research: Academic vs. non-academic information
- The research process
- Creating a research plan
- Primary and secondary sources
- Academic vs. non-academic information
- Evaluating information: The PAARC test
Identifying academic journal articles
There is a huge amount of information available from many different sources for your research. There is also great variety in the quality of the material that you find. Some of the information comes from reliable sources, but other information comes from questionable sources. To produce high-quality research papers, you must rely on information from authoritative sources, such as academic articles. An excellent way to ensure that you are working with authoritative information is to work with academic (also often called "scholarly" or "peer reviewed") sources.
How can you be sure that information that you have found is an academic article? Here are seven guidelines to help you identify one:
1. Authorship
- The author of the article is an expert in their field. Often, the author’s title and/or qualifications are indicated after their name in the article. This is also true if there are multiple authors of an article.
2. Peer Reviewed
- The article has undergone the peer-review process. This means that the article that you are reading has been reviewed by a panel of experts in the field (peers of the author), and that the research has been deemed worthy of publication in the journal. Most journal databases will allow you to refine your results to only display articles that have undergone peer review.
3. Bibliography/List of References/Works Cited
- The article has a bibliography, list of references, or works cited. The author of the article will cite his or her references at the end of the article. This allows the reader to see what information that author has referred to in his or her article. By doing this, the author is giving proper credit to the work or others , but also helping to build their case.
- Generally, the article has more than five pages. The length of the article is important because it indicates to the reader that it is a serious piece of work, and that in-depth research has been done by the author. While there are articles that can be published in academic journals that are 5 pages or less, these do not usually represent in-depth research.
- The writing style is theoretical rather than practical. The theoretical perspective means that a contribution to the existing body of research in the field is being made.
6. Audience
- The intended audience of the article is scholars, researchers, and other professionals in the field. An academic article is not generally intended for readers outside the subject field.
- Which the exception of academic work dealing directly with works or art or directly discussing imagery, there are no photos or other images included as part of an academic article. Even when photos are included, they are strictly there to illustrate the research being presented in the work, and will be referenced directly. Depending on the subject matter, there may be graphs or charts that support the author’s research. Page layouts are usually very plain, and do not include colour embellishments or other design flourishes.
- << Previous: Primary and secondary sources
- Next: Evaluating information: The PAARC test >>
- Last Updated: Feb 26, 2024 11:05 AM
- URL: https://libguides.marianopolis.edu/research

- Experimental Vs Non-Experimental Research: 15 Key Differences

There is a general misconception around research that once the research is non-experimental, then it is non-scientific, making it more important to understand what experimental and experimental research entails. Experimental research is the most common type of research, which a lot of people refer to as scientific research.
Non experimental research, on the other hand, is easily used to classify research that is not experimental. It clearly differs from experimental research, and as such has different use cases.
In this article, we will be explaining these differences in detail so as to ensure proper identification during the research process.
What is Experimental Research?
Experimental research is the type of research that uses a scientific approach towards manipulating one or more control variables of the research subject(s) and measuring the effect of this manipulation on the subject. It is known for the fact that it allows the manipulation of control variables.
This research method is widely used in various physical and social science fields, even though it may be quite difficult to execute. Within the information field, they are much more common in information systems research than in library and information management research.
Experimental research is usually undertaken when the goal of the research is to trace cause-and-effect relationships between defined variables. However, the type of experimental research chosen has a significant influence on the results of the experiment.
Therefore bringing us to the different types of experimental research. There are 3 main types of experimental research, namely; pre-experimental, quasi-experimental, and true experimental research.
Pre-experimental Research
Pre-experimental research is the simplest form of research, and is carried out by observing a group or groups of dependent variables after the treatment of an independent variable which is presumed to cause change on the group(s). It is further divided into three types.
- One-shot case study research
- One-group pretest-posttest research
- Static-group comparison
Quasi-experimental Research
The Quasi type of experimental research is similar to true experimental research, but uses carefully selected rather than randomized subjects. The following are examples of quasi-experimental research:
- Time series
- No equivalent control group design
- Counterbalanced design.
True Experimental Research
True experimental research is the most accurate type, and may simply be called experimental research. It manipulates a control group towards a group of randomly selected subjects and records the effect of this manipulation.
True experimental research can be further classified into the following groups:
- The posttest-only control group
- The pretest-posttest control group
- Solomon four-group
Pros of True Experimental Research
- Researchers can have control over variables.
- It can be combined with other research methods.
- The research process is usually well structured.
- It provides specific conclusions.
- The results of experimental research can be easily duplicated.
Cons of True Experimental Research
- It is highly prone to human error.
- Exerting control over extraneous variables may lead to the personal bias of the researcher.
- It is time-consuming.
- It is expensive.
- Manipulating control variables may have ethical implications.
- It produces artificial results.
What is Non-Experimental Research?
Non-experimental research is the type of research that does not involve the manipulation of control or independent variable. In non-experimental research, researchers measure variables as they naturally occur without any further manipulation.
This type of research is used when the researcher has no specific research question about a causal relationship between 2 different variables, and manipulation of the independent variable is impossible. They are also used when:
- subjects cannot be randomly assigned to conditions.
- the research subject is about a causal relationship but the independent variable cannot be manipulated.
- the research is broad and exploratory
- the research pertains to a non-causal relationship between variables.
- limited information can be accessed about the research subject.
There are 3 main types of non-experimental research , namely; cross-sectional research, correlation research, and observational research.
Cross-sectional Research
Cross-sectional research involves the comparison of two or more pre-existing groups of people under the same criteria. This approach is classified as non-experimental because the groups are not randomly selected and the independent variable is not manipulated.
For example, an academic institution may want to reward its first-class students with a scholarship for their academic excellence. Therefore, each faculty places students in the eligible and ineligible group according to their class of degree.
In this case, the student’s class of degree cannot be manipulated to qualify him or her for a scholarship because it is an unethical thing to do. Therefore, the placement is cross-sectional.
Correlational Research
Correlational type of research compares the statistical relationship between two variables .Correlational research is classified as non-experimental because it does not manipulate the independent variables.
For example, a researcher may wish to investigate the relationship between the class of family students come from and their grades in school. A questionnaire may be given to students to know the average income of their family, then compare it with CGPAs.
The researcher will discover whether these two factors are positively correlated, negatively corrected, or have zero correlation at the end of the research.
Observational Research
Observational research focuses on observing the behavior of a research subject in a natural or laboratory setting. It is classified as non-experimental because it does not involve the manipulation of independent variables.
A good example of observational research is an investigation of the crowd effect or psychology in a particular group of people. Imagine a situation where there are 2 ATMs at a place, and only one of the ATMs is filled with a queue, while the other is abandoned.
The crowd effect infers that the majority of newcomers will also abandon the other ATM.
You will notice that each of these non-experimental research is descriptive in nature. It then suffices to say that descriptive research is an example of non-experimental research.
Pros of Observational Research
- The research process is very close to a real-life situation.
- It does not allow for the manipulation of variables due to ethical reasons.
- Human characteristics are not subject to experimental manipulation.
Cons of Observational Research
- The groups may be dissimilar and nonhomogeneous because they are not randomly selected, affecting the authenticity and generalizability of the study results.
- The results obtained cannot be absolutely clear and error-free.
What Are The Differences Between Experimental and Non-Experimental Research?
- Definitions
Experimental research is the type of research that uses a scientific approach towards manipulating one or more control variables and measuring their defect on the dependent variables, while non-experimental research is the type of research that does not involve the manipulation of control variables.
The main distinction in these 2 types of research is their attitude towards the manipulation of control variables. Experimental allows for the manipulation of control variables while non-experimental research doesn’t.
Examples of experimental research are laboratory experiments that involve mixing different chemical elements together to see the effect of one element on the other while non-experimental research examples are investigations into the characteristics of different chemical elements.
Consider a researcher carrying out a laboratory test to determine the effect of adding Nitrogen gas to Hydrogen gas. It may be discovered that using the Haber process, one can create Nitrogen gas.
Non-experimental research may further be carried out on Ammonia, to determine its characteristics, behaviour, and nature.
There are 3 types of experimental research, namely; experimental research, quasi-experimental research, and true experimental research. Although also 3 in number, non-experimental research can be classified into cross-sectional research, correlational research, and observational research.
The different types of experimental research are further divided into different parts, while non-experimental research types are not further divided. Clearly, these divisions are not the same in experimental and non-experimental research.
- Characteristics
Experimental research is usually quantitative, controlled, and multivariable. Non-experimental research can be both quantitative and qualitative , has an uncontrolled variable, and also a cross-sectional research problem.
The characteristics of experimental research are the direct opposite of that of non-experimental research. The most distinct characteristic element is the ability to control or manipulate independent variables in experimental research and not in non-experimental research.
In experimental research, a level of control is usually exerted on extraneous variables, therefore tampering with the natural research setting. Experimental research settings are usually more natural with no tampering with the extraneous variables.
- Data Collection/Tools
The data used during experimental research is collected through observational study, simulations, and surveys while non-experimental data is collected through observations, surveys, and case studies. The main distinction between these data collection tools is case studies and simulations.
Even at that, similar tools are used differently. For example, an observational study may be used during a laboratory experiment that tests how the effect of a control variable manifests over a period of time in experimental research.
However, when used in non-experimental research, data is collected based on the researcher’s discretion and not through a clear scientific reaction. In this case, we see a difference in the level of objectivity.
The goal of experimental research is to measure the causes and effects of variables present in research, while non-experimental research provides very little to no information about causal agents.
Experimental research answers the question of why something is happening. This is quite different in non-experimental research, as they are more descriptive in nature with the end goal being to describe what .
Experimental research is mostly used to make scientific innovations and find major solutions to problems while non-experimental research is used to define subject characteristics, measure data trends, compare situations and validate existing conditions.
For example, if experimental research results in an innovative discovery or solution, non-experimental research will be conducted to validate this discovery. This research is done for a period of time in order to properly study the subject of research.
Experimental research process is usually well structured and as such produces results with very little to no errors, while non-experimental research helps to create real-life related experiments. There are a lot more advantages of experimental and non-experimental research , with the absence of each of these advantages in the other leaving it at a disadvantage.
For example, the lack of a random selection process in non-experimental research leads to the inability to arrive at a generalizable result. Similarly, the ability to manipulate control variables in experimental research may lead to the personal bias of the researcher.
- Disadvantage
Experimental research is highly prone to human error while the major disadvantage of non-experimental research is that the results obtained cannot be absolutely clear and error-free. In the long run, the error obtained due to human error may affect the results of the experimental research.
Some other disadvantages of experimental research include the following; extraneous variables cannot always be controlled, human responses can be difficult to measure, and participants may also cause bias.
In experimental research, researchers can control and manipulate control variables, while in non-experimental research, researchers cannot manipulate these variables. This cannot be done due to ethical reasons.
For example, when promoting employees due to how well they did in their annual performance review, it will be unethical to manipulate the results of the performance review (independent variable). That way, we can get impartial results of those who deserve a promotion and those who don’t.
Experimental researchers may also decide to eliminate extraneous variables so as to have enough control over the research process. Once again, this is something that cannot be done in non-experimental research because it relates more to real-life situations.
Experimental research is carried out in an unnatural setting because most of the factors that influence the setting are controlled while the non-experimental research setting remains natural and uncontrolled. One of the things usually tampered with during research is extraneous variables.
In a bid to get a perfect and well-structured research process and results, researchers sometimes eliminate extraneous variables. Although sometimes seen as insignificant, the elimination of these variables may affect the research results.
Consider the optimization problem whose aim is to minimize the cost of production of a car, with the constraints being the number of workers and the number of hours they spend working per day.
In this problem, extraneous variables like machine failure rates or accidents are eliminated. In the long run, these things may occur and may invalidate the result.
- Cause-Effect Relationship
The relationship between cause and effect is established in experimental research while it cannot be established in non-experimental research. Rather than establish a cause-effect relationship, non-experimental research focuses on providing descriptive results.
Although it acknowledges the causal variable and its effect on the dependent variables, it does not measure how or the extent to which these dependent variables change. It, however, observes these changes, compares the changes in 2 variables, and describes them.
Experimental research does not compare variables while non-experimental research does. It compares 2 variables and describes the relationship between them.
The relationship between these variables can be positively correlated, negatively correlated or not correlated at all. For example, consider a case whereby the subject of research is a drum, and the control or independent variable is the drumstick.
Experimental research will measure the effect of hitting the drumstick on the drum, where the result of this research will be sound. That is, when you hit a drumstick on a drum, it makes a sound.
Non-experimental research, on the other hand, will investigate the correlation between how hard the drum is hit and the loudness of the sound that comes out. That is, if the sound will be higher with a harder bang, lower with a harder bang, or will remain the same no matter how hard we hit the drum.
- Quantitativeness
Experimental research is a quantitative research method while non-experimental research can be both quantitative and qualitative depending on the time and the situation where it is been used. An example of a non-experimental quantitative research method is correlational research .
Researchers use it to correlate two or more variables using mathematical analysis methods. The original patterns, relationships, and trends between variables are observed, then the impact of one of these variables on the other is recorded along with how it changes the relationship between the two variables.
Observational research is an example of non-experimental research, which is classified as a qualitative research method.
- Cross-section
Experimental research is usually single-sectional while non-experimental research is cross-sectional. That is, when evaluating the research subjects in experimental research, each group is evaluated as an entity.
For example, let us consider a medical research process investigating the prevalence of breast cancer in a certain community. In this community, we will find people of different ages, ethnicities, and social backgrounds.
If a significant amount of women from a particular age are found to be more prone to have the disease, the researcher can conduct further studies to understand the reason behind it. A further study into this will be experimental and the subject won’t be a cross-sectional group.
A lot of researchers consider the distinction between experimental and non-experimental research to be an extremely important one. This is partly due to the fact that experimental research can accommodate the manipulation of independent variables, which is something non-experimental research can not.
Therefore, as a researcher who is interested in using any one of experimental and non-experimental research, it is important to understand the distinction between these two. This helps in deciding which method is better for carrying out particular research.
Connect to Formplus, Get Started Now - It's Free!
- examples of experimental research
- non experimental research
- busayo.longe
You may also like:
Simpson’s Paradox & How to Avoid it in Experimental Research
In this article, we are going to look at Simpson’s Paradox from its historical point and later, we’ll consider its effect in...
What is Experimenter Bias? Definition, Types & Mitigation
In this article, we will look into the concept of experimental bias and how it can be identified in your research
Response vs Explanatory Variables: Definition & Examples
In this article, we’ll be comparing the two types of variables, what they both mean and see some of their real-life applications in research
Experimental Research Designs: Types, Examples & Methods
Ultimate guide to experimental research. It’s definition, types, characteristics, uses, examples and methodolgy
Formplus - For Seamless Data Collection
Collect data the right way with a versatile data collection tool. try formplus and transform your work productivity today..
Advertisement
Research vs. non-research universities: knowledge sharing and research engagement among academicians
- Published: 18 September 2021
- Volume 24 , pages 25–39, ( 2023 )
Cite this article

- Muhammad Ashraf Fauzi ORCID: orcid.org/0000-0003-2137-4602 1 , 2
1016 Accesses
11 Citations
2 Altmetric
Explore all metrics
This study investigated the differences in knowledge sharing (KS) behavior among academicians from research universities (RUs) and non-research universities (Non-RUs) and the impact of their differences on research engagement in Malaysia. From the lens of the theory of planned behavior, research engagement is integrated into the original theory as the consequence of KS behavior. Applying a multi-group analysis through partial least square structural equation modeling, 458 academic staff from twenty public universities in Malaysia participated in the study. The study findings revealed that in the RU sample, commitment and subjective norm have no significant impact on attitude and intention, respectively. However, a significant impact of commitment and subjective norm on attitude and intention, respectively, was found in the non-RU sample. This study contributes to the knowledge management perspective among academicians and compares RU and non-RU academicians in Malaysia. A relevant mitigation plan must be taken to ensure that academicians in both RUs and non-RUs share their knowledge willingly and sincerely to elevate the status of higher education in the country to a greater height as a top world-class university. Moreover, an analysis of the implication of higher education in the country as well as institutionalization of education excellence could be achieved through better KS behavior in the South East Asian region.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
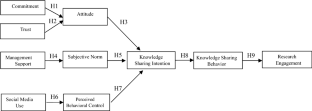
Similar content being viewed by others

Factors influencing knowledge sharing intention at a university: evidence from Zimbabwean academics
Enhancing knowledge sharing and research collaboration among academics: the role of knowledge management.

Factors Affecting Knowledge Sharing Intention Among Academic Staff
Ajzen, I. (1991). The theory of planned behavior. Organizational Behaviour and Human Decision Processes, 50 , 179–211. https://doi.org/10.1016/0749-5978(91)90020-T
Article Google Scholar
Ajzen, I. (2011). The theory of planned behaviour: Reactions and reflections. Psychology and Health, 26 (9), 1113–1127. https://doi.org/10.1080/08870446.2011.613995
Akhavan, P. S., Hosseini, S. M., Abbasi, M., & Manteghi, M. (2015). Knowledge sharing determinants, behaviours, and innovative work behaviours. Aslib Journal of Information Management, 67 (5), 562–591. https://doi.org/10.1108/AJIM-02-2015-0018
Akosile, A., & Olatokun, W. (2020). Factors influencing knowledge sharing among academics in Bowen University, Nigeria. Journal of Librarianship and Information Science, 52 (2), 410–427. https://doi.org/10.1177/0961000618820926
Al-Husseini, S., El Beltagi, I., & Moizer, J. (2019). Transformational leadership and innovation: The mediating role of knowledge sharing amongst higher education faculty. International Journal of Leadership in Education, 22 (2), 1–24. https://doi.org/10.1080/13603124.2019.1588381
Al-Kurdi, O. F., El-Haddadeh, R., & Eldabi, T. (2020). The role of organizational climate in managing knowledge sharing among academics in higher education. International Journal of Information Management, 50 , 217–227. https://doi.org/10.1016/j.ijinfomgt.2019.05.018
Allen, N. J., & Meyer, J. P. (1990). The measurement and antecedents of affective, continuance and normative commitment to the organization. Journal of Occupational Psychology, 63 , 1–18. https://doi.org/10.1111/j.2044-8325.1990.tb00506.x
Altbach, P. G. (2012). The globalization of college and university rankings. Change, 44 (1), 26–31.
Bock, G., Zmud, R., Kim, Y., & Lee, J. (2005). Behavioral intention formation in knowledge sharing: Examining the roles of extrinsic motivators, social-psychological forces, and organizational climate. MIS Quarterly, 29 (1), 87–111. https://doi.org/10.2307/25148669
Borg, S., & Alshumaimeri, Y. (2012). University teacher educators’ research engagement: Perspectives from Saudi Arabia. Teaching and Teacher Education, 28 (3), 347–356. https://doi.org/10.1016/j.tate.2011.10.011
Chandran, D., & Alammari, A. M. (2020). Influence of culture on knowledge sharing attitude among academic staff in elearning virtual communities in Saudi Arabia. Information Systems Frontiers . https://doi.org/10.1007/s10796-020-10048-x
Chang, C. M., Hsu, M. H., & Lee, Y. J. (2015). Factors influencing knowledge-sharing behavior in virtual communities: A longitudinal investigation. Information Systems Management, 32 (4), 331–340. https://doi.org/10.1080/10580530.2015.1080002
Chatterjee, S., Rana, N. P., & Dwivedi, Y. K. (2020). Social media as a tool of knowledge sharing in academia: An empirical study using valance, instrumentality and expectancy (VIE) approach. Journal of Knowledge Management., 24 (10), 2531–2552. https://doi.org/10.1108/JKM-04-2020-0252
Cheah, J. H., Ng, S. I., Ting, H., Memon, M. A., & Loo, S. C. S. (2019). Customer orientation and office space performance: Assessing the moderating effect of building grade using PLS-MGA. International Journal of Strategic Property Management, 23 (2), 117–129. https://doi.org/10.3846/ijspm.2019.7437
Chin, W. W. (2010). How to write up and report PLS analyses. Handbook of partial least squares (pp. 655–690). Berlin: Springer.
Chapter Google Scholar
Dijkstra, T. K., & Henseler, J. (2011). Linear indices in nonlinear structural equation models: Best fitting proper indices and other composites. Quality & Quantity, 45 (6), 1505–1518. https://doi.org/10.1007/s11135-010-9359-z
Dobrota, M., Bulajic, M., Bornmann, L., & Jeremic, V. (2016). A new approach to the QS university ranking using the composite I-distance indicator: Uncertainty and sensitivity analyses. Journal of the Association for Information Science and Technology, 67 (1), 200–211. https://doi.org/10.1002/asi.23355
Dusdal, J., Powell, J. J., Baker, D. P., Fu, Y. C., Shamekhi, Y., & Stock, M. (2020). University vs research institute? The dual pillars of German science production, 1950–2010. Minerva, 58 (3), 319–342. https://doi.org/10.1007/s11024-019-09393-2
Elrehail, H., Emeagwali, O. L., Alsaad, A., & Alzghoul, A. (2018). The impact of transformational and authentic leadership on innovation in higher education: The contingent role of knowledge sharing. Telematics and Informatics, 35 (1), 55–67. https://doi.org/10.1016/j.tele.2017.09.018
Farid, H., Izadi, Z., Ismail, I. A., & Alipour, F. (2015). Relationship between quality of work life and organizational commitment among lecturers in a Malaysian public research university. The Social Science Journal, 52 (1), 54–61. https://doi.org/10.1016/j.soscij.2014.09.003
Fauzi, M. A., Nya-Ling, C. T., Thurasamy, R., & Ojo, A. O. (2018). An integrative model of knowledge sharing in Malaysian higher learning institute. Kybernetes, 47 (5), 1031–1052. https://doi.org/10.1108/K-10-2017-0388
Fauzi, M. A., Nya-Ling, C. T., Thursamy, R., & Ojo, A. O. (2019). Knowledge sharing: Role of academics towards research productivity in higher learning institution. VINE Journal of Information and Knowledge Management Systems., 49 (1), 136–159. https://doi.org/10.1108/VJIKMS-09-2018-0074
Fauzi, M. A., Tan, C. N. L., Daud, M., & Awalludin, M. M. N. (2020). University rankings: A review of methodological flaws. Issues in Educational Research, 30 (1), 79–96.
Google Scholar
Fullwood, R., & Rowley, J. (2017). An investigation of factors affecting knowledge sharing amongst UK academics. Journal of Knowledge Management., 21 (5), 1254–1271. https://doi.org/10.1108/JKM-07-2016-0274
Fussy, D. S. (2018). Policy directions for promoting university research in Tanzania. Studies in Higher Education, 43 (9), 1573–1585. https://doi.org/10.1080/03075079.2016.1266611
García-Sánchez, P., Díaz-Díaz, N. L., & De Saá-Pérez, P. (2019). Social capital and knowledge sharing in academic research teams. International Review of Administrative Sciences, 85 (1), 191–207. https://doi.org/10.1177/0020852316689140
Ghazali, E. M., Mutum, D. S., Pua, M. H. J., & Ramayah, T. (2020). Status-quo satisfaction and smartwatch adoption: A multi-group analysis. Industrial Management & Data Systems., 120 (12), 2319–2347. https://doi.org/10.1108/IMDS-10-2019-0576
Goh, S. K., & Sandhu, M. S. (2013). Knowledge sharing among Malaysian academics: Influence of affective commitment and trust. Electronic Journal of Knowledge Management, 11 (1), 38–48.
Gold, A. H., & Arvind Malhotra, A. H. S. (2001). Knowledge management: An organizational capabilities perspective. Journal of Management Information Systems, 18 (1), 185–214. https://doi.org/10.1080/07421222.2001.11045669
Guide, V. D. R., Jr., & Ketokivi, M. (2015). Notes from the editors: Redefining some methodological criteria for the journal. Journal of Operations Management, 37 , v–viii.
Hair, J. F., Jr., Hult, G. T. M., Ringle, C. M., & Sarstedt, M. (2017). A primer on partial least squares structural equation modeling (PLS-SEM) . Sage Publications Inc.
Hayhoe, R. (2019). The gift of Indian higher learning traditions to the global research university. Asia Pacific Journal of Education, 39 (2), 177–189. https://doi.org/10.1080/02188791.2019.1621799
Henseler, J., Ringle, C. M., & Sarstedt, M. (2015). A new criterion for assessing discriminant validity in variance-based structural equation modeling. Journal of the Academy of Marketing Science, 43 (1), 115–135. https://doi.org/10.1007/s11747-014-0403-8
Henseler, J., Ringle, C. M., & Sarstedt, M. (2016). Testing measurement invariance of composites using partial least squares. International Marketing Review., 33 (3), 405–431. https://doi.org/10.1108/IMR-09-2014-0304
Hung, S. Y., Lai, H. M., & Chou, Y. C. (2015). Knowledge-sharing intention in professional virtual communities: A comparison between posters and lurkers. Journal of the Association for Information Science and Technology, 66 (12), 2494–2510. https://doi.org/10.1002/asi.23339
Hussein, A. T. T., Singh, S. K., Farouk, S., & Sohal, A. S. (2016). Knowledge sharing enablers, processes and firm innovation capability. Journal of Workplace Learning, 28 (8), 484–495. https://doi.org/10.1108/JWL-05-2016-0041
Iqbal, A., Latif, F., Marimon, F., Sahibzada, U. F., & Hussain, S. (2019). From knowledge management to organizational performance. Journal of Enterprise Information Management, 32 (1), 36–59. https://doi.org/10.1108/JEIM-04-2018-0083
Iqbal, M. J., Rasli, A., Heng, L. H., Ali, M. B. B., Hassan, I., & Jolaee, A. (2011). Academic staff knowledge sharing intentions and university innovation capability. African Journal of Business Management, 5 (27), 11051–11059.
Jolaee, A., Nor, K. M., Khani, N., & Yusoff, R. M. (2014). Factors affecting knowledge sharing intention among academic staff. International Journal of Educational Management., 28 (4), 413–431. https://doi.org/10.1108/IJEM-03-2013-0041
Khan, D., & Ali, N. (2019). Knowledge sharing concept, attitude and influencing factors: A case with Indian academic librarians. Journal of Information & Knowledge Management, 18 (03), 1950034. https://doi.org/10.1142/S0219649219500345
Kline, R. B. (2011). Principles and practice of structural equation modeling . Guilford Publications Press.
Kock, N., & Lynn, G. (2012). Lateral collinearity and misleading results in variance-based SEM: An illustration and recommendations. Journal of the Association for Information Systems, 13 (7), 546–580.
Lee, J. C., Shiue, Y. C., & Chen, C. Y. (2016). Examining the impacts of organizational culture and top management support of knowledge sharing on the success of software process improvement. Computers in Human Behavior, 54 , 462–474. https://doi.org/10.1016/j.chb.2015.08.030
Lin, T. C., Chang, C. L. H., & Tsai, W. C. (2016). The influences of knowledge loss and knowledge retention mechanisms on the absorptive capacity and performance of a MIS department. Management Decision, 54 (7), 1757–1787. https://doi.org/10.1108/MD-02-2016-0117
Lo, M. F., Tian, F., & Ng, P. M. L. (2021). Top management support and knowledge sharing: the strategic role of affiliation and trust in academic environment. Journal of Knowledge Management . https://doi.org/10.1108/JKM-10-2020-0800
Lombardi, S., Cavaliere, V., Giustiniano, L., & Cipollini, F. (2020). What money cannot buy: The detrimental effect of rewards on knowledge sharing. European Management Review, 17 (1), 153–170. https://doi.org/10.1111/emre.12346
MacKenzie, S. B., & Podsakoff, P. M. (2012). Common method bias in marketing: Causes, mechanisms, and procedural remedies. Journal of Retailing, 88 (4), 542–555. https://doi.org/10.1016/j.jretai.2012.08.001
Mafabi, S., Nasiima, S., Muhimbise, E. M., Kasekende, F., & Nakiyonga, C. (2017). The mediation role of intention in knowledge sharing behavior. VINE Journal of Information and Knowledge Management Systems., 47 (2), 172–193. https://doi.org/10.1108/VJIKMS-02-2016-0008
Matthews, L. (2017). Applying multi-group analysis in PLS-SEM: A step-by-step process. Partial least squares path modeling (pp. 219–243). Springer.
McAllister, D. J. (1995). Affect-and cognition-based trust as foundations for interpersonal cooperation in organizations. Academy of Management Journal, 38 (1), 24–59. https://doi.org/10.5465/256727
Ministry of Higher Education Malaysia (MOHE) (2017). Enhancing University Transformation Programme, Silver Book Academic and Cost Efficiency, Putrajaya.
Punniyamoorthy, M., & Asumptha, J. A. (2019). A study on knowledge sharing behavior among academicians in India. Knowledge Management & E-Learning, 11 (1), 95–113. https://doi.org/10.34105/j.kmel.2019.11.006
Rahman, M. S., Mannan, M., Hossain, M. A., Zaman, M. H., & Hassan, H. (2018). Tacit knowledge-sharing behavior among the academic staff. International Journal of Educational Management., 32 (5), 761–782. https://doi.org/10.1108/IJEM-08-2017-0193
Ramayah, T., Yeap, J. A., & Ignatius, J. (2013). An empirical inquiry on knowledge sharing among academicians in higher learning institutions. Minerva, 51 (2), 131–154. https://doi.org/10.1007/s11024-013-9229-7
Rasoolimanesh, S. M., Ringle, C. M., Jaafar, M., & Ramayah, T. (2017). Urban vs. rural destinations: Residents’ perceptions, community participation and support for tourism development. Tourism Management, 60 , 147–158. https://doi.org/10.1016/j.tourman.2016.11.019
Robertson, D. L., & Pelaez, M. (2016). Behavior analytic concepts and change in a large metropolitan research university: The graduation success initiative. Journal of Organizational Behavior Management, 36 (2–3), 123–153. https://doi.org/10.1080/01608061.2016.1200513
Saide, S., Indrajit, R. E., Trialih, R., Ramadhani, S., & Najamuddin, N. (2019). A theoretical and empirical validation of information technology and path-goal leadership on knowledge creation in university: Leaders support and social media trend. Journal of Science and Technology Policy Management, 10 (3), 551–568. https://doi.org/10.1108/JSTPM-06-2018-0067
Sveiby, K., & Simons, R. (2002). Collaborative climate and effectiveness of knowledge work-an empirical study. Journal of Knowledge Management, 6 (5), 420–433. https://doi.org/10.1108/13673270210450388
Tan, C. N. L. (2016). Enhancing knowledge sharing and research collaboration among academics: The role of knowledge management. Higher Education, 71 (4), 525–556. https://doi.org/10.1007/s10734-015-9922-6
Thien, L. M., & Jamil, H. (2020). Students as ‘Customers’: Unmasking course experience and satisfaction of undergraduate students at a Malaysian Research University. Journal of Higher Education Policy and Management, 42 (5), 579–600. https://doi.org/10.1080/1360080X.2019.1660045
Thong, J. Y. L., Hong, W., & Tam, K. (2002). Understanding user acceptance of digital libraries: What are the roles of interface characteristics, organizational context, and individual differences? International Journal Human Computer Studies, 57 , 215–242. https://doi.org/10.1016/S1071-5819(02)91024-4
Thoreson, R. W., Kardash, C. M., Leuthold, D. A., & Morrow, K. A. (1990). Gender differences in the academic career. Research in Higher Education, 31 (2), 193–209. https://doi.org/10.1007/BF00992262
Times Higher Education (TIMES) (2021). Times Higher Education World University Rankings. Retrieved May 12, 2021, from https://www.timeshighereducation.com/world-university-rankings/2021/world-ranking#!/page/0/length/25/sort_by/rank/sort_order/asc/cols/stats
Tseng, F. C., & Kuo, F. Y. (2014). A study of social participation and knowledge sharing in the teachers’ online professional community of practice. Computers & Education, 72 , 37–47. https://doi.org/10.1016/j.compedu.2013.10.005
Urbach, N., & Ahlemann, F. (2010). Structural equation modeling in information systems research using partial least squares. Journal of Information Technology Theory and Application, 11 (2), 5–40.
Wu, I.-L., & Chen, J.-L. (2005). An extension of trust and TAM model with TPB in the initial adoption of online tax: An empirical study. International Journal of Human-Computer Studies, 62 , 784–808. https://doi.org/10.1016/j.ijhcs.2005.03.003
Download references
Author information
Authors and affiliations.
Faculty of Industrial Management, Universiti Malaysia Pahang, Gambang, Malaysia
Muhammad Ashraf Fauzi
Centre for Software Development and Integrated Computing, Universiti Malaysia Pahang, Gambang, Malaysia
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Muhammad Ashraf Fauzi .
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
See Table 6
Rights and permissions
Reprints and permissions
About this article
Fauzi, M.A. Research vs. non-research universities: knowledge sharing and research engagement among academicians. Asia Pacific Educ. Rev. 24 , 25–39 (2023). https://doi.org/10.1007/s12564-021-09719-4
Download citation
Received : 25 May 2021
Revised : 11 September 2021
Accepted : 13 September 2021
Published : 18 September 2021
Issue Date : March 2023
DOI : https://doi.org/10.1007/s12564-021-09719-4
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Knowledge sharing
- Higher education
- Research University
- Research engagement
- Find a journal
- Publish with us
- Track your research

Difference Between Experimental and Non-Experimental Research
When designing research , you must take into account the different methods and experimental research types that are available.
There are two main types of research: non-experimental and experimental. It’s critical to understand the advantages and disadvantages of each type in order to choose which is best for your research goals.
Experimental research is a type of quantitative research that controls the variables in order to test a hypothesis. Non-experimental research does not control the variables but instead looks at naturally occurring factors without manipulating them to test a hypothesis.
This article explains more about the benefits and drawbacks of experimental versus non-experimental research so you can decide which one is right for your project.
- Table of Contents
What is Experimental Research?
Experimental research is a scientific method where the researcher manipulates the variables in the experiment to see how this influences the findings. In experimental research, the research subject(s) are subjected to one or more manipulations of their control variables while the effects of these manipulations are being monitored. Because it enables the adjustment of control variables, it is well known.
The goal of the experiment is to test a hypothesis . The data collected during the experiment will help you understand how accurate your hypothesis is.
Experiments are a type of quantitative research that aims to control all the variables in order to accurately test a hypothesis. Experiments are typically used in social sciences such as psychology, economics, or sociology. Other fields like biology also use experimental research, but they often use a different method called “controlled laboratory experiments”.
Experiments are also used in business research , but businesses often employ a different type of experimental research called “field experiments”.
What is Non-Experimental Research?
Non-experimental research does not experimentally manipulate the variables directly. Instead, it looks at naturally occurring factors without experimenting with them. Research that is non-experimental does not manipulate a control variable or an independent variable. In non-experimental research, variables are measured as they are without any additional manipulation.
These types of research are usually quantitative because they don’t manipulate the variables, but they don’t employ the same experimental approach as an experiment. To conduct non-experimental research, you must first define the population that you want to study. Then, you would take sample data from that population to find out what the results are.
The goal of non-experimental research is to find out what naturally occurs in the environment without directly manipulating anything. This means that the researcher does not change any variables during the research process. Non-experimental research is often used in fields like social sciences or economics where it is hard to experimentally manipulate the variables.
Benefits of Experimental Research
Experimental research has several advantages.
- First, it allows you to control many different factors to test the accuracy of your hypothesis. This means that you can completely control the outcome of your research if you use the right methods.
- Experimental research also allows you to conduct the research in a short amount of time, meaning you can get accurate results quickly. This is important for businesses that need to make quick decisions about products or services.
- Experimental research often leads to the creation of new products or solutions because researchers can test multiple solutions at the same time. Many businesses use experimental research to create new products or services because it allows them to test different variables that would otherwise be difficult to control in a non-experimental research setting.
Disadvantages of Experimental Research
Experimental research does come with a few disadvantages.
- First, it can be very expensive to conduct and may require specialized equipment or employees. You also need to hire professionals to create a hypothesis and conduct the experiment.
- Experimental research can also be time consuming. You must create the right conditions to ensure that the right variables are being tested. This can take a long time.
- Experimental research can also be difficult to control. If you don’t have the right conditions, you may not get accurate results. Researchers also have to make sure that other factors don’t influence the outcome of the experiment.
- Experimental research can also lead to inaccurate findings if the researcher makes a mistake or if the conditions are not right for the experiment.
- Academic Research vs Industry Research
- Best Research Methodology Books for Researchers and Academics
- Clinical Research vs Lab Research
- Difference Between a Research Lab and Hospital Lab
- Difference Between One-tailed and Two-tailed Test
- Difference between Mediator and Moderator
- Difference Between Research Article and Research Paper
Benefits of Non-Experimental Research
- Non-experimental research does not have the same financial or time requirements as experimental research. You can conduct non-experimental research with minimal resources and you don’t need to create a hypothesis in order to conduct it. This means that you don’t have to hire specialists or spend as much money as you would on an experiment.
- Non-experimental research is also easier to control than an experiment because you don’t have to create a controlled setting. Instead, you simply observe what naturally occurs in the environment. This means that you don’t have to worry about outside factors influencing the outcome of the research.
- Non-experimental research is also less risky than an experiment because you don’t have to worry about making a mistake. If something goes wrong during the research, you don’t have to start the experiment over again. Instead, you can simply make a note of it and continue with the research .
Disadvantages of Non-Experimental Research
Non-experimental research does have a few disadvantages.
- First, it does not allow you to test your hypothesis as accurately as experimental research does. This means that you don’t really know if your product or idea will work in the real world.
- Non-experimental research is also limited by the number of variables that are naturally occurring in the environment. This means that you might not be able to find the right data or factors to test your hypothesis.
- If you want to test a lot of different variables at once, non-experimental research can become difficult to conduct. You must then separate the data in order to find out which factor is influencing your findings.
The primary difference between these two forms of research is how they approach manipulating control variables. Non-experimental research does not allow for the manipulation of control variables.
Example: Experimental vs Non-Experimental Research
Laboratory experiments in which various chemical elements are mixed together to observe how one element affects another are instances of experimental research, whereas studies into the properties of various chemical elements are examples of non-experimental research.
Which Type of Research is Right for You?
When choosing between experimental and non-experimental research, you should remember that both methods have their benefits and drawbacks. No one research method is better than the other. Instead, different research types are better for different projects.
You should choose experimental research if you want to test a hypothesis as accurately as possible. This type of research is good for testing new products or services because you can control the variables directly.
You should choose non-experimental research if you want to observe naturally occurring factors. This type of research is good for projects where you can’t experimentally manipulate the variables or where it’s difficult to do so.
Other articles
Please read through some of our other articles with examples and explanations if you’d like to learn more about research methodology.
Comparision
- Basic and Applied Research
- Cross-Sectional vs Longitudinal Studies
- Survey vs Questionnaire
- Open Ended vs Closed Ended Questions
- Experimental and Non-Experimental Research
- Inductive vs Deductive Approach
- Null and Alternative Hypothesis
- Reliability vs Validity
- Population vs Sample
- Conceptual Framework and Theoretical Framework
- Bibliography and Reference
- Stratified vs Cluster Sampling
- Sampling Error vs Sampling Bias
- Internal Validity vs External Validity
- Full-Scale, Laboratory-Scale and Pilot-Scale Studies
- Plagiarism and Paraphrasing
- Research Methodology Vs. Research Method
- Mediator and Moderator
- Type I vs Type II error
- Descriptive and Inferential Statistics
- Microsoft Excel and SPSS
- Parametric and Non-Parametric Test
- Independent vs. Dependent Variable – MIM Learnovate
- Research Article and Research Paper
- Proposition and Hypothesis
- Principal Component Analysis and Partial Least Squares
- Research Lab and Hospital Lab
- Thesis Statement and Research Question
- Quantitative Researchers vs. Quantitative Traders
- Premise, Hypothesis and Supposition
- Survey Vs Experiment
- Hypothesis and Theory
- Independent vs. Dependent Variable
- APA vs. MLA
- Ghost Authorship vs. Gift Authorship
- Research Methods
- Quantitative Research
- Qualitative Research
- Case Study Research
- Survey Research
- Conclusive Research
- Descriptive Research
- Cross-Sectional Research
- Theoretical Framework
- Conceptual Framework
- Triangulation
- Grounded Theory
- Quasi-Experimental Design
- Mixed Method
- Correlational Research
- Randomized Controlled Trial
- Stratified Sampling
- Ethnography
- Ghost Authorship
- Secondary Data Collection
- Primary Data Collection
- Ex-Post-Facto
- Dissertation Topic
- Thesis Statement
- Research Proposal
- Research Questions
- Research Problem
- Research Gap
- Types of Research Gaps
- Operationalization of Variables
- Literature Review
- Research Hypothesis
- Questionnaire
- Reliability
- Measurement of Scale
- Sampling Techniques
- Acknowledgements
- PLS-SEM model
- Principal Components Analysis
- Multivariate Analysis
- Friedman Test
- Chi-Square Test (Χ²)
- Effect Size
- Directional vs. Non-Directional Hypothesis

Misbah Rashid, an expert in Technology Management, holds an MBA and an MS in Information Systems and Technology Management. She has experience teaching marketing and technology in business at the university level.
Related Posts
Survey sampling: what it is, types & tips, cluster sampling | method and examples, who is a good peer reviewer, peer review | types of peer review, ethics in research: safeguarding integrity and credibility, advantages and disadvantages of snowball sampling, exploring qualitative researcher skills: what they are and how to develop them, difference between quota sampling and stratified sampling, how effective laboratory design impacts health, safety, and productivity, why is laboratory safety important in research.
Comments are closed.

- school Campus Bookshelves
- menu_book Bookshelves
- perm_media Learning Objects
- login Login
- how_to_reg Request Instructor Account
- hub Instructor Commons
Margin Size
- Download Page (PDF)
- Download Full Book (PDF)
- Periodic Table
- Physics Constants
- Scientific Calculator
- Reference & Cite
- Tools expand_more
- Readability
selected template will load here
This action is not available.
1.11: Experimental and non-experimental research
- Last updated
- Save as PDF
- Page ID 16762

- Matthew J. C. Crump
- Brooklyn College of CUNY
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
One of the big distinctions that you should be aware of is the distinction between “experimental research” and “non-experimental research”. When we make this distinction, what we’re really talking about is the degree of control that the researcher exercises over the people and events in the study.
Experimental research
The key features of experimental research is that the researcher controls all aspects of the study, especially what participants experience during the study. In particular, the researcher manipulates or varies something (IVs), and then allows the outcome variable (DV) to vary naturally. The idea here is to deliberately vary the something in the world (IVs) to see if it has any causal effects on the outcomes. Moreover, in order to ensure that there’s no chance that something other than the manipulated variable is causing the outcomes, everything else is kept constant or is in some other way “balanced” to ensure that they have no effect on the results. In practice, it’s almost impossible to think of everything else that might have an influence on the outcome of an experiment, much less keep it constant. The standard solution to this is randomization : that is, we randomly assign people to different groups, and then give each group a different treatment (i.e., assign them different values of the predictor variables). We’ll talk more about randomization later in this course, but for now, it’s enough to say that what randomization does is minimize (but not eliminate) the chances that there are any systematic difference between groups.
Let’s consider a very simple, completely unrealistic and grossly unethical example. Suppose you wanted to find out if smoking causes lung cancer. One way to do this would be to find people who smoke and people who don’t smoke, and look to see if smokers have a higher rate of lung cancer. This is not a proper experiment, since the researcher doesn’t have a lot of control over who is and isn’t a smoker. And this really matters: for instance, it might be that people who choose to smoke cigarettes also tend to have poor diets, or maybe they tend to work in asbestos mines, or whatever. The point here is that the groups (smokers and non-smokers) actually differ on lots of things, not just smoking. So it might be that the higher incidence of lung cancer among smokers is caused by something else, not by smoking per se. In technical terms, these other things (e.g. diet) are called “confounds”, and we’ll talk about those in just a moment.
In the meantime, let’s now consider what a proper experiment might look like. Recall that our concern was that smokers and non-smokers might differ in lots of ways. The solution, as long as you have no ethics, is to control who smokes and who doesn’t. Specifically, if we randomly divide participants into two groups, and force half of them to become smokers, then it’s very unlikely that the groups will differ in any respect other than the fact that half of them smoke. That way, if our smoking group gets cancer at a higher rate than the non-smoking group, then we can feel pretty confident that (a) smoking does cause cancer and (b) we’re murderers.
Non-experimental research
Non-experimental research is a broad term that covers “any study in which the researcher doesn’t have quite as much control as they do in an experiment”. Obviously, control is something that scientists like to have, but as the previous example illustrates, there are lots of situations in which you can’t or shouldn’t try to obtain that control. Since it’s grossly unethical (and almost certainly criminal) to force people to smoke in order to find out if they get cancer, this is a good example of a situation in which you really shouldn’t try to obtain experimental control. But there are other reasons too. Even leaving aside the ethical issues, our “smoking experiment” does have a few other issues. For instance, when I suggested that we “force” half of the people to become smokers, I must have been talking about starting with a sample of non-smokers, and then forcing them to become smokers. While this sounds like the kind of solid, evil experimental design that a mad scientist would love, it might not be a very sound way of investigating the effect in the real world. For instance, suppose that smoking only causes lung cancer when people have poor diets, and suppose also that people who normally smoke do tend to have poor diets. However, since the “smokers” in our experiment aren’t “natural” smokers (i.e., we forced non-smokers to become smokers; they didn’t take on all of the other normal, real life characteristics that smokers might tend to possess) they probably have better diets. As such, in this silly example they wouldn’t get lung cancer, and our experiment will fail, because it violates the structure of the “natural” world (the technical name for this is an “artifactual” result; see later).
One distinction worth making between two types of non-experimental research is the difference between quasi-experimental research and case studies . The example I discussed earlier – in which we wanted to examine incidence of lung cancer among smokers and non-smokers, without trying to control who smokes and who doesn’t – is a quasi-experimental design. That is, it’s the same as an experiment, but we don’t control the predictors (IVs). We can still use statistics to analyse the results, it’s just that we have to be a lot more careful.
The alternative approach, case studies, aims to provide a very detailed description of one or a few instances. In general, you can’t use statistics to analyse the results of case studies, and it’s usually very hard to draw any general conclusions about “people in general” from a few isolated examples. However, case studies are very useful in some situations. Firstly, there are situations where you don’t have any alternative: neuropsychology has this issue a lot. Sometimes, you just can’t find a lot of people with brain damage in a specific area, so the only thing you can do is describe those cases that you do have in as much detail and with as much care as you can. However, there’s also some genuine advantages to case studies: because you don’t have as many people to study, you have the ability to invest lots of time and effort trying to understand the specific factors at play in each case. This is a very valuable thing to do. As a consequence, case studies can complement the more statistically-oriented approaches that you see in experimental and quasi-experimental designs. We won’t talk much about case studies in these lectures, but they are nevertheless very valuable tools!
- Open access
- Published: 14 May 2024
Research outcomes informing the selection of public health interventions and strategies to implement them: A cross-sectional survey of Australian policy-maker and practitioner preferences
- Luke Wolfenden 1 , 2 , 3 ,
- Alix Hall 1 , 2 , 3 ,
- Adrian Bauman 1 , 4 , 5 ,
- Andrew Milat 6 , 7 ,
- Rebecca Hodder 1 , 2 , 3 ,
- Emily Webb 1 ,
- Kaitlin Mooney 1 ,
- Serene Yoong 1 , 2 , 3 , 8 , 9 ,
- Rachel Sutherland 1 , 2 , 3 &
- Sam McCrabb 1 , 2 , 3
Health Research Policy and Systems volume 22 , Article number: 58 ( 2024 ) Cite this article
245 Accesses
7 Altmetric
Metrics details
A key role of public health policy-makers and practitioners is to ensure beneficial interventions are implemented effectively enough to yield improvements in public health. The use of evidence to guide public health decision-making to achieve this is recommended. However, few studies have examined the relative value, as reported by policy-makers and practitioners, of different broad research outcomes (that is, measures of cost, acceptability, and effectiveness). To guide the conduct of research and better inform public health policy and practice, this study aimed at describing the research outcomes that Australian policy-makers and practitioners consider important for their decision-making when selecting: (a) public health interventions; (b) strategies to support their implementation; and (c) to assess the differences in research outcome preferences between policy-makers and practitioners.
An online value-weighting survey was conducted with Australian public health policy-makers and practitioners working in the field of non-communicable disease prevention. Participants were presented with a list of research outcomes and were asked to select up to five they considered most critical to their decision-making. They then allocated 100 points across these – allocating more points to outcomes perceived as more important. Outcome lists were derived from a review and consolidation of evaluation and outcome frameworks in the fields of public health knowledge translation and implementation. We used descriptive statistics to report relative preferences overall and for policy-makers and practitioners separately.
Of the 186 participants; 90 primarily identified as policy-makers and 96 as public health prevention practitioners. Overall, research outcomes of effectiveness, equity, feasibility, and sustainability were identified as the four most important outcomes when considering either interventions or strategies to implement them. Scores were similar for most outcomes between policy-makers and practitioners.
For Australian policy-makers and practitioners working in the field of non-communicable disease prevention, outcomes related to effectiveness, equity, feasibility, and sustainability appear particularly important to their decisions about the interventions they select and the strategies they employ to implement them. The findings suggest researchers should seek to meet these information needs and prioritize the inclusion of such outcomes in their research and dissemination activities. The extent to which these outcomes are critical to informing the decision of policy-makers and practitioners working in other jurisdictions or contexts warrants further investigation.
Peer Review reports
Research evidence has a key role in public health policy-making [ 1 ]. Consideration of research is important to maximize the potential impact of investments in health policies and services. Public health policy-makers and practitioners frequently seek out research to inform their professional decision-making [ 2 ]. However, they report that published research is not well aligned with their evidence needs [ 3 , 4 ]. Public health decision-making is a complex and dynamic process where evidence is used in a variety of ways, and for different purposes [ 3 , 5 , 6 ]. Ensuring research meets the evidence needs of public health policy-makers and practitioners is, therefore, an important strategy to improve its use in decision-making [ 7 , 8 , 9 , 10 ].
“Research outcomes” are broad domains or constructs measured to evaluate the impacts of health policies, practices or interventions, such as their effectiveness or acceptability. They are distinct from “outcome measures”, which are the measures selected to assess an outcome. Outcome measures require detailed specification of measurement parameters, including the measurement techniques and instrument, and consideration of the suitability of its properties (for example, validity) given the research question. The inclusion of research outcomes considered most relevant to public health policy-makers and practitioners is one way in which researchers can support evidence-informed decision-making.
Policy-makers are primarily responsible for developing public health policy and selecting and resourcing health programs. Practitioners are primarily responsible for supporting their implementation. As such, public health policy-makers and practitioners require research to: (i) help identify “what works” to guide the selection of interventions that will be beneficial for their community, for example, those that are effective in improving health, and acceptable to the target population and/or (ii) to help identify “how to implement” effective intervention, for example, strategies that are capable of achieving implementation at a level sufficient to accrue benefit, are affordable and reach the targeted population [ 6 , 11 ]. Research that includes outcomes relevant to these responsibilities facilitates evidence-informed decision-making by public health policy-makers and practitioners.
Initiatives such as the World Health Organization INTEGRATe Evidence (WHO INTEGRATE) framework [ 12 ], and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) Evidence to Decision framework [ 13 ] have been designed to support the selection of public health interventions. Application of these frameworks required the collation and synthesis of a range of scientific evidence including studies employing qualitative and quantitative research designs. Collectively, the frameworks suggest public health policy-makers and practitioners should consider, alongside research outcomes reporting the effectiveness of a public health intervention, other research outcomes such as cost–effectiveness, potential harms and acceptability of an intervention to patients or community.
Several authors have also sought to guide outcomes researchers should include in implementation studies [ 11 ]. Proctor and colleagues defined a range of implementation research outcomes [distinct from service or clinical (intervention) effectiveness outcomes] – including intervention adoption, appropriateness, feasibility, fidelity, cost, penetration and sustainability [ 14 ]. This work helped standardize how the field of implementation science defined, measured and reported implementation outcomes. More recently McKay and colleagues put forward measures of implementation “determinants” and “outcomes” and proposed a “minimum set” of such outcomes to include in implementation and scale-up studies. The implementation research outcomes proposed by both Proctor and McKay and colleagues were developed primarily from the input of researchers to improving the quality and consistency of reporting in implementation science. However, the relative value of these outcomes to the decision-making of public health policy-makers, and in particular practitioners, has largely been unexplored.
While several studies have explored policy-maker and practitioner research evidence preferences, these have focused on a small number of potential outcomes [ 15 , 16 , 17 ]. An appraisal of the potential value, and importance of a comprehensive range of research outcomes to public health policy-maker and practitioner decision-making, therefore, is warranted. In this study, we sought to quantify the relative importance of research outcomes from the perspective of Australian public health policy-makers and practitioners working in the field of non-communicable disease prevention (hereafter referred to as “prevention” policy-makers or practitioners). Specifically, using a value-weighting methodology to elicit relative preferences, the study aimed to describe: (a) research the outcomes prevention policy-makers and practitioners regard as important to their decision-making when selecting a public health intervention to address an identified health issue, (b), research the outcomes prevention policy-makers and practitioners regard as important to their decision-making when selecting a strategy to support the implementation of a public health intervention in the community and (c) assess the differences between prevention policy-makers and practitioners regarding their research outcome preferences.
Design and setting
An online cross-sectional value-weighting survey was conducted with Australian public health prevention policy-makers and practitioners. This study was undertaken as one step of a broader program of work to establish a core outcome set that has been prospectively registered on the Core Outcome Measures in Effectiveness Trials (COMET database; https://www.comet-initiative.org/Studies/Details/1791 ).
Participant eligibility
To be eligible, participants had to self-identify as having worked as a public health prevention policy-maker or practitioner at a government or non-government health organization within the past 5 years. While the term “policy-maker” has been used to describe legislators in US studies, in Australian research it has broadly been used to describe employees of government departments (or non-government agencies) involved in the development of public health policy [ 18 , 19 , 20 , 21 , 22 ]. Policy-makers are not typically involved in the direct implementation of policy or the delivery of health services. We defined a “policy-maker” as a professional who makes decisions, plans and actions that are undertaken to achieve specific public health prevention goals on behalf of a government or non-government organization [ 23 ]. Practitioners are typically employed by government or non-government organizations responsible for prevention service provision, and are directly involved in the implementation or supporting the implementation of public health policies or programs. Specifically, we defined a “practitioner” as a professional engaged in the delivery of public health prevention programs, implementing services or models of care in health and community settings (definition developed by research team). Research and evaluation are a core competency of the public health prevention workforce in Australia [ 24 ], as it is in other countries [ 25 ]. As such, participants may be engaged in research and have published research studies. Researchers, such as those employed by academic institutions only and without an explicit public health policy or practice role in a policy or practice organization, were excluded.
Recruitment
Comprehensive methods were used to recruit individuals through several agencies. First, email invitations were distributed to Australian government health agencies at local (for example, New South Wales Local Health District Population Health units), state (for example, departments or ministries of health) and national levels, as well as to non-government organizations (for example, Cancer Council) and professional societies (for example, Public Health Association Australia). Registered practitioners with the International Union for Health Promotion and Education (IUHPE) from Australia were contacted by public domain emails or on LinkedIn (where identified) with the study invitation. Authors who had published articles of relevant topics from 2018 to 2021 within three Australian public health journals [ Australian and New Zealand Journal of Public Health ( ANZJPH ), Health Promotion Journal of Australia ( HPJA ) and Public Health Research and Practice ( PHRP )] were invited to participate in the study. Invitation emails included links to the information statement for participants and the online survey. The online survey was also promoted on the social media account of a partnering organization [National Centre of Implementation Science (NCOIS)] as well as on Twitter and LinkedIn. From these social media accounts individuals could self-select to participate in the online survey. Reminder emails were sent to non-responders at approximately 2 and 4 weeks following the initial email invitation.
Data collection and measures
The online survey was kept on servers at the Hunter Medical Research Institute, New South Wales, Australia, and deployed using the REDCap software [ 26 ], a secured web-based application for building and managing online surveys and databases. The length of the survey was approximately 20–30 min in duration.
Professional characteristics
Participants completed brief items assessing their professional role (that is, practitioner or policy-maker), the number of years’ experience as policy-makers or practitioners, their professional qualifications and the prevention risk factors (for example, smoking, nutrition, physical activity, injury, sexual health, etc.) for which they had expertise.
Valued intervention and implementation outcomes
We sought to identify outcomes that may be valued by public health policy-makers and practitioners when making decisions about what policies and/or programs of interventions to implement and how implementation could best occur. We separated outcomes on this basis, consistent with recommendations of the evidence policy and practice [ 27 ], the effectiveness–implementation research typology [ 28 , 29 ] and trial conduct and reporting guidelines [ 30 ]. This is illustrated in a broad study logic model (Fig. 1 ).

Both effective interventions and effective implementation are required to improve health outcomes
The authors undertook a review of intervention- and implementation-relevant outcome frameworks to determine program and intervention outcomes that may be of interest to policy-makers and practitioners, including the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) Framework [ 31 , 32 ], the Intervention Scalability Assessment Tool (ISAT) [ 18 ] and Proctor and colleagues’ implementation outcome definitions [ 14 ] as well as a series of publications on the topic [ 31 , 33 , 34 , 35 , 36 , 37 , 38 , 39 , 40 , 41 , 42 , 43 ]. This was used to generate a comprehensive inventory of all possible outcomes (and outcome definitions) that may be of interest to public health policy-makers and practitioners. The outcome list was then reduced following grouping of outcomes addressing similar constructs or concepts. A panel of 16 public health policy-makers provided feedback on their perceived importance of each outcome for evidence-informed policy and practice decision-making, as well as the proposed outcome definition. This process occurred over two rounds until no further suggested improvements or clarifications were provided or requested, yielding a final list of 17 outcomes to inform the selection of public health intervention and 16 outcomes for the selection of implementation strategies (Additional file 1 : Table S1). Panel participants also pre-tested the survey instrument; however, they were not invited to participate in the value-weighting study.
Participating public health policy-makers and practitioners completed the value-weighting survey. Value-weighting surveys offer advantages over other methods to identify preferences (such as ranks or mean scores on a rating scale), as they provide an opportunity to quantify the relative preference or value of different dissemination strategies from the perspective of public health policy-makers or practitioners. Specifically, they were only presented with the list of outcomes and their definition, and were asked to select up to 5 of the 17 interventions “that they considered are critical to their decision-making when selecting a public health intervention to address an identified health issue” and 16 implementation outcomes “that they consider to be critical to their decision-making when selecting a strategy to support the implementation of a public health intervention in the community” in a decision-making context. Participants were then asked to value weight, allocating 100 points across their five (or less) intervention and implementation outcomes. A higher allocation of points represented a greater level of perceived importance. In this way, participants weight the allocation of points to outcomes based on preference. No statistical weights are applied in the analysis. Participants were asked to select up to five outcomes as this restriction forced a prioritization of the outcomes among participants. The identification of a small number of critical outcomes, rather than all relevant outcomes, is also recommended to facilitate research outcome harmonization [ 44 , 45 ].
Statistical analysis
All statistical analyses and data management were undertaken in SAS version 9.3. Descriptive statistics were used to describe the study sample. Similar to other value-weighting studies, we used descriptive analyses to identify the intervention and implementation outcomes ranked from highest to lowest importance [ 46 , 47 ]. Items not selected or allocated any points were assumed a score of 0, to reflect that they were not perceived as a high-priority outcome by the participant. Specifically, the mean points allocated to each of the individual outcomes were calculated and ranked in descending order. This was calculated overall for the entire participant sample, as well as separately by policy-makers and practitioners. As points were assigned in free-text fields, in instances where participants allocated more or less than 100 points across the individual items, the points they allocated were standardized to 100. Differences in the points allocated to each individual outcome by policy-maker/practitioner role were explored using Mann–Whitney U test. To examine any differences in the outcome preferences by participant risk factor expertise, we also examined and described outcome preferences among risk factor subgroups (with a combined sample of > 30 participants). These findings are discussed.
A total of 186 eligible participants completed the survey in part or in full.
Of the 186 participants, 90 primarily identified as policy-makers and 96 as public health prevention practitioners (Table 1 ). In all, 37% of participants (47% policy-makers, 27% practitioners) had over 15 years’ experience, and approximately one third (32% policy-makers, 36% practitioners) had a PhD. The most common areas of experience were nutrition and dietetics (38% policy-maker, 53% practitioner), physical activity or sedentary behaviour (46% policy-maker, 44% practitioner), obesity (49% policy-maker, 48% practitioner) and tobacco, alcohol or other drugs (51% policy-maker, 34% practitioner).
Valued outcomes
Intervention outcomes.
A total of 169 participants (83 policy-makers and 86 practitioners, with 7 and 10 missing, respectively) responded to the value-weighting questions for the 17 listed intervention outcomes. Table 2 (Fig. 2 ) reports the mean and standard deviation of points allocated by policy-makers and practitioners for each outcome, ranked in descending order to represent the most to least important. For policy-makers and practitioners combined, the effectiveness of an intervention, and its impact on equity, were clearly identified by participants as the leading two outcomes, with a mean allocation of 24.47 [standard deviation (SD) = 17.43] and 13.44(SD = 12.80), respectively. The mean scores for outcomes of feasibility (9.78) and sustainability (9.04) that ranked third and fourth, respectively, were similar; then scores dropped noticeably to 7.24 for acceptability and 5.81 for economic outcomes.

Line graph representing mean points allocated for the 17 intervention outcomes overall and by role
For most outcomes, average scores were similar for policy-makers and practitioners. However, practitioner scores for the outcome of acceptability (mean = 8.95, SD = 9.11), which ranked third most important for practitioners was significantly different than for policy-makers (mean = 5.48, SD = 9.62), where it was ranked seventh ( p = 0.005). Economics/cost outcomes were ranked fifth by policy-makers (mean = 8.28, SD = 10.63), which significantly differed from practitioners (mean = 3.43, SD = 6.56), where it was ranked ninth ( p = 0.002). For co-benefits, ranked eighth by policy-makers (mean = 4.37, SD = 7.78), scores were significantly different than for practitioners (mean = 2.27, SD = 6.49), where it was ranked thirteenth ( p = 0.0215). Rankings for the top five outcomes were identical for those with expertise in nutrition and dietetics, physical activity or sedentary behaviour, obesity and tobacco, alcohol or other drugs (Additional file 1 : Table S2).
Implementation outcomes
A total of 153 participants (75 policy-makers and 78 practitioners, with 15 and 18 missing, respectively) responded to the value-weighting questions for the 16 listed implementation outcomes (Table 3 , Fig. 3 ). The effectiveness of an implementation strategy was clearly identified by participants as the most important intervention outcome, with a mean allocation of 19.82 (SD = 16.85) overall. The mean scores for the next three ranked outcomes namely equity (mean = 10.42, SD = 12.7), feasibility (mean = 10.2, SD = 12.91) and sustainability (mean = 10.08, SD = 10.58) were similar, and thereafter, scores noticeably dropped for measures of adoption (mean = 8.55, SD = 10.90), the fifth-ranked outcome.

Line graph representing mean points allocated for the 16 implementation outcomes overall and by role
For most implementation outcomes (Fig. 3 ) policy-makers and practitioners scores were similar. However, economics outcomes were ranked seventh for policy-makers with a mean = 5.58 (SD = 9.25), compared with practitioners who had a ranking of eleventh for this outcome (mean = 2.88, SD = 6.67). The difference in the points allocated were statistically significant between the two groups ( p = 0.0439). Timeliness was ranked tenth most important for policy-makers, with a mean allocation of 4.03 (SD = 7.72), compared with practitioners who had a ranking of fourteenth for this outcome and a mean allocation of 2.05 (SD = 5.78). The difference in mean scores between policy-makers and practitioners on this outcome was not significant. Rankings and scores were similar for those with expertise in nutrition and dietetics, physical activity or sedentary behaviour, obesity and tobacco, alcohol or other drugs (Additional file 1 : Table S3).
Broadly, this study sought to better understand the information valued by public health policy-makers and practitioners to support their decisions regarding what and how interventions should be implemented in the community. The most valued research outcomes were the same regardless of whether policy-makers or practitioners were selecting interventions or implementation strategies. Namely outcomes regarding the effectiveness of interventions and implementation strategies. Following this, outcomes about equity, feasibility and sustainability also appeared to represent priorities. The study also found broad convergence among the most valued research outcomes, between policy-makers and practitioners, and across participants with expertise across different non-communicable disease (NCD) risk factors (for example, nutrition, obesity and tobacco). Such findings underscore the importance of research reporting these outcomes to support the translation of public health research into policy and practice.
For outcomes about decisions regarding intervention selection, the findings are broadly consistent with factors recommended by evidence-to-decision frameworks. For example, the top six ranked outcomes (effectiveness, equity, feasibility, sustainability, acceptability and economic), are also represented in both the WHO INTEGRATE framework [ 12 ] and the GRADE Evidence to Decision framework [ 13 ]. However, research outcomes about harms (adverse effects), which are included in both the WHO INTEGRATE and GRADE frameworks were ranked 13th by participants in this study. Such a finding was surprising given that potential benefits and harms of an intervention must be considered to appraise its net impact on patient or public health. Health professionals, however, do not have accurate expectations of the harms and benefits of therapeutic interventions. This appears particularly to be the case for public health professionals who acknowledge the potential for unintended consequences of policies [ 48 ] but consider these risks to be minimal [ 49 ]. The findings, therefore, may reflect the tendency of health professionals to overestimate the benefits of therapeutic interventions, and to a larger extent, underestimate harms [ 50 , 51 ]. In doing so, participants may have elevated their reported value of outcomes regarding the beneficial effectiveness of an intervention and discounted their value of outcomes reporting potential harms. Further research is warranted to substantiate this hypothesis, or explore whether other factors such as participant comprehension or misinterpretation of the outcome description may explain the finding. Nonetheless, the inclusion of measures of adverse effects (or harms) as trial outcomes is prudent to support evidence-informed public health decision-making, as is the use of strategies to facilitate risk communication to ensure the likelihood of such outcomes is understood by policy-makers and practitioners [ 52 , 53 , 54 ].
To our knowledge, this is the first study to examine the research evidence needs of public health policy-makers and practitioners when deciding on what strategies may be used to support policy or program implementation. Most of the eight implementation outcomes recommended by Proctor and colleagues [ 14 ] were ranked within the top eight by participants of this study. However, equity outcomes, ranked second by these participants, were not an outcome included in the list of outcomes defined by Proctor and colleagues. The findings may reflect public health values, which, as a discipline, has equity at its core [ 55 ]. It may also reflect the increasing attention to issues of health equity in implementation science [ 56 ].
Further, one of the eight Proctor outcomes, penetration – defined by Proctor and colleagues as the integration or saturation of an intervention within a service setting and its subsystems – was not ranked highly. Successful penetration implies a level of organization institutionalization of an intervention, which once achieved may continue to provide ongoing benefit to patients or populations. It may also suggest the capacity within the organization to expand implementation or adopt new interventions. Penetration outcomes, therefore, have been suggested to be particularly important to model and understand the potential impact of investment of scarce health resources in the implementation of public health policies and interventions [ 57 ].
At face value, such findings may suggest, at least from the perspective of public health policy-makers and practitioners, that penetration outcomes may not be particularly valued in terms of decision-making. However, it may also reflect a lack of familiarity with this term among public health policy-makers and practitioners, where related outcomes such as “reach” are more commonly used in the literature [ 14 , 58 ]. Alternatively it may be due to the conceptual similarity of this and other outcomes such as adoption, maintenance or sustainability. In other studies, for example, penetration has been operationalized to include the product of “reach”, “adoption” and “organizational maintenance” [ 58 ]. A lack of clear conceptual distinction may have led some participants to allocate points to related outcomes such as “adoption” rather than “penetration”.
The use of concept mapping techniques, consolidation of definitions of existing outcomes, and articulation of specific measures aligned to these outcomes may reduce some of these conceptual challenges. Indeed, best practice processes to develop core outcome sets for clinical trials suggest processes of engagement with end-users [ 45 ], stakeholders and researchers to articulate both broad outcomes and specific measures of these to support a shared understanding of important outcomes (and measures) to be included in such research. For example, there are many measures and economic methods to derive related to a broad outcome of “cost” (for example, absolute costs, cost–effectiveness, cost–benefit, cost–utility, and budget impact analysis) [ 59 ]. However, public health policy-makers’ preference or perceived value of these different measures to their decision-making will likely vary. While work in the field to map or align specific measures to broad outcomes is ongoing [ 57 , 58 , 60 ], extending this to empirically investigate end-user preferences for measures would be an important contribution to the field.
Broadly speaking, there was little variation in the outcomes valued between policy-makers and practitioners. However, economic evaluations were ranked as more important by policy-makers. The findings may reflect differences in the roles of Australian public health policy-makers and practitioners. That is, government policy-makers are often responsible for setting and financing the provision of public health programs, whereas health practitioners are responsible for directly supporting or undertaking their delivery. Economic considerations, therefore, may have greater primacy among policy-makers, who may be more likely to incur program costs [ 19 ]. Further research to explore and better understand these areas of divergence is warranted.
The study intended to provide information about outcomes that were generally of most use in public health policy and practice decision-making. However, such decisions are often highly contextual, and preferences may vary depending on the policy-maker or practitioner, the health issue to be addressed, the target population or broader decision-making circumstances [ 2 , 61 ]. As such, the extent to which the findings reported in this study generalize to other contexts, such as those working in different fields of public health, on different health issues or from countries or jurisdictions outside Australia is unknown. Future research examining the outcome preferences of public health policy-makers and practitioners in different contexts, therefore, is warranted.
The contextual nature of evidence needs of policy-makers and practitioners may explain, in part, the variability in outcome preferences. In many cases, for example, the mean of the outcome preference was less than its standard deviation. The interpretation of the study findings should consider this variability. That is, there is little distinguishing the mean preference ranks of many outcomes. However, the study findings at the extremes are unambiguous, suggesting clear preferences for the highest over the lowest ranking outcomes that did not differ markedly across policy-makers, practitioners or those with expertise in addressing different non-communicable disease risks such as nutrition, physical activity or tobacco or alcohol use.
Several study limitations are worth considering when interpreting the research findings. The initial inventory of outcomes was compiled from outcome frameworks, many of which were generic health or medical research outcomes that are uncommon in public health prevention research. There was considerable overlap in the outcomes included across frameworks, though how these were defined at times varied. Variability in outcome terminology has previously been identified as a problem for the field [ 62 ]. Despite being provided definitions for each, some participants may have responded to survey items based on their pre-existing understanding of these terms. Furthermore, following completion of the study, a programming error was identified whereby the definition of “Acceptability of the implementation strategy” was incorrectly assigned as “A measure of the uptake or reach of an implementation strategy”. The extent to which this may have influenced participant preferences is unclear, so sensitivity analysis was conducted by removing all participants who selected acceptability as a measure of interest. We conducted two analyses, one where the people who chose acceptability were removed but their other rankings remained and another where all their data were deleted. Results indicated that the top five outcomes did not differ after conducting the analysis, with only sustainability moving from fourth to second place in the second sensitivity analysis (Additional file 1 : Tables S4 and S5).
The pathway from research production to research in health policy or practice is complex. While a range of effective public health policies and interventions exist across a range of community settings [ 63 , 64 , 65 , 66 ], their implementation at a level capable of achieving population-level risk reductions remains elusive [ 67 , 68 , 69 , 70 ]. Nonetheless, undertaking research with end-use in mind, including reporting of outcomes valued by decision-makers, will likely facilitate the knowledge translation process [ 7 ]. In this study we found that outcomes related to effectiveness, equity, feasibility and sustainability appear important to decisions policy-makers and practitioners make about the interventions they select and the strategies they employ to implement public health prevention initiatives. Researchers interested in supporting evidence-informed decision-making should seek to provide for these information needs and prioritize such outcomes in dissemination activities to policy-makers and practitioners.
Contribution to the literature
It is essential to the research needs of policy-makers and practitioners to determine core outcomes to facilitate research use and knowledge translation.
Here we quantify the relative values of a variety of research outcomes commonly used in health research.
Findings suggest the primary outcomes of interest to public health prevention policy-makers and practitioners when making decisions about the selection of interventions and strategies to implement them are related to effectiveness, equity, feasibility and sustainability and that these do not differ markedly between public health prevention policy-makers and practitioners.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
Australian and New Zealand Journal of Public Health
Health Promotion Journal of Australia
Intervention scalability assessment tool
Non-communicable disease
National Centre of Implementation Science
Public Health Research and Practice
World Health Organization
Campbell D, Moore G, Sax Institute. Increasing the use of research in policymaking. An Evidence Check rapid review brokered by the Sax Institute for the NSW Ministry of Health. 2017. https://www.health.nsw.gov.au/research/Documents/increasing-the-use-of-research.pdf .
Oliver KA, de Vocht F. Defining “evidence” in public health: a survey of policymakers’ uses and preferences. Eur J Public Health. 2017;27(2):112–7. https://doi.org/10.1093/eurpub/ckv082 .
Article PubMed Google Scholar
Newson RS, Rychetnik L, King L, Milat AJ, Bauman AE. Looking for evidence of research impact and use: a qualitative study of an Australian research-policy system. Res Eval. 2021;30(4):458–69. https://doi.org/10.1093/reseval/rvab017 .
Article Google Scholar
van der Graaf P, Cheetham M, McCabe K, Rushmer R. Localising and tailoring research evidence helps public health decision making. Health Info Libr J. 2018;35(3):202–12. https://doi.org/10.1111/hir.12219 .
World Health Organization. Evidence, policy, impact: WHO guide for evidence-informed decision-making. World Health Organization; 2021.
Global Commission on Evidence to Address Societal Challenges. The Evidence Commission Report: a wake-up call and path forward for decisionmakers, evidence intermediaries, and impact-oriented evidence producers. 2022. https://www.mcmasterforum.org/networks/evidence-commission/report/english .
Wolfenden L, Mooney K, Gonzalez S, et al. Increased use of knowledge translation strategies is associated with greater research impact on public health policy and practice: an analysis of trials of nutrition, physical activity, sexual health, tobacco, alcohol and substance use interventions. Health Res Policy Syst. 2022;20(1):15. https://doi.org/10.1186/s12961-022-00817-2 .
Article PubMed PubMed Central Google Scholar
Kathy E, David G, Anne H, et al. Improving knowledge translation for increased engagement and impact in healthcare. BMJ Open Qual. 2020;9(3): e000983. https://doi.org/10.1136/bmjoq-2020-000983 .
Squires JE, Santos WJ, Graham ID, et al. Attributes and features of context relevant to knowledge translation in health settings: a response to recent commentaries. Int J Health Policy Management. 2023;12(1):1–4. https://doi.org/10.34172/ijhpm.2023.7908 .
Thomas A, Bussières A. Leveraging knowledge translation and implementation science in the pursuit of evidence informed health professions education. Adv Health Sci Educ Theory Pract. 2021;26(3):1157–71. https://doi.org/10.1007/s10459-020-10021-y .
Dobbins M, Jack S, Thomas H, Kothari A. Public health decision-makers’ informational needs and preferences for receiving research evidence. Worldviews Evid-Based Nurs. 2007;4(3):156–63. https://doi.org/10.1111/j.1741-6787.2007.00089.x .
Rehfuess EA, Stratil JM, Scheel IB, Portela A, Norris SL, Baltussen R. The WHO-INTEGRATE evidence to decision framework version 10: integrating WHO norms and values and a complexity perspective. BMJ Glob Health. 2019;4(Suppl 1):e000844. https://doi.org/10.1136/bmjgh-2018-000844 .
Moberg J, Oxman AD, Rosenbaum S, et al. The GRADE Evidence to Decision (EtD) framework for health system and public health decisions. Health Res Policy Syst. 2018;16(1):45. https://doi.org/10.1186/s12961-018-0320-2 .
Proctor E, Silmere H, Raghavan R, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38(2):65–76. https://doi.org/10.1007/s10488-010-0319-7 .
Dodson EA, Geary NA, Brownson RC. State legislators’ sources and use of information: bridging the gap between research and policy. Health Educ Res. 2015;30(6):840–8. https://doi.org/10.1093/her/cyv044 .
Morshed AB, Dodson EA, Tabak RG, Brownson RC. Comparison of research framing preferences and information use of state legislators and advocates involved in cancer control, United States, 2012–2013. Prev Chronic Dis. 2017;14:E10. https://doi.org/10.5888/pcd14.160292 .
Turon H, Wolfenden L, Finch M, et al. Dissemination of public health research to prevent non-communicable diseases: a scoping review. BMC Public Health. 2023;23(1):757. https://doi.org/10.1186/s12889-023-15622-x .
Milat A, Lee K, Conte K, et al. Intervention Scalability Assessment Tool: a decision support tool for health policy makers and implementers. Health Res Policy Syst. 2020;18(1):1–17.
Milat AJ, King L, Newson R, et al. Increasing the scale and adoption of population health interventions: experiences and perspectives of policy makers, practitioners, and researchers. Health Res Policy Syst. 2014;12(1):18. https://doi.org/10.1186/1478-4505-12-18 .
Cleland V, McNeilly B, Crawford D, Ball K. Obesity prevention programs and policies: practitioner and policy-maker perceptions of feasibility and effectiveness. Obesity. 2013;21(9):E448–55. https://doi.org/10.1002/oby.20172 .
Wolfenden L, Bolsewicz K, Grady A, et al. Optimisation: defining and exploring a concept to enhance the impact of public health initiatives. Health Res Policy Syst. 2019;17(1):108. https://doi.org/10.1186/s12961-019-0502-6 .
Purtle J, Dodson EA, Nelson K, Meisel ZF, Brownson RC. Legislators’ sources of behavioral health research and preferences for dissemination: variations by political party. Psychiatr Serv. 2018;69(10):1105–8. https://doi.org/10.1176/appi.ps.201800153 .
World Health Organization. WHO Health policy [Internet] 2019;
Australian Health Promotion Association Core competencies for health promotion practitioners. Maroochydore: University of the Sunshine Coast. 2009;
Barry MM, Battel-Kirk B, Dempsey C. The CompHP Core Competencies Framework for Health Promotion in Europe. Health Educ Behav. 2012;39(6):648–62. https://doi.org/10.1177/1090198112465620 .
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81. https://doi.org/10.1016/j.jbi.2008.08.010 .
Wolfenden L, Williams CM, Kingsland M, et al. Improving the impact of public health service delivery and research: a decision tree to aid evidence-based public health practice and research. Aust N Zeal J Public Health. 2020;44(5):331–2. https://doi.org/10.1111/1753-6405.13023 .
Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50(3):217–26. https://doi.org/10.1097/MLR.0b013e3182408812 .
Wolfenden L, Williams CM, Wiggers J, Nathan N, Yoong SL. Improving the translation of health promotion interventions using effectiveness–implementation hybrid designs in program evaluations. Health Promot J Austr. 2016;27(3):204–7. https://doi.org/10.1071/HE16056 .
Wolfenden L, Foy R, Presseau J, et al. Designing and undertaking randomised implementation trials: guide for researchers. Br Med J. 2021;372:m3721. https://doi.org/10.1136/bmj.m3721 .
Suhonen R, Papastavrou E, Efstathiou G, et al. Patient satisfaction as an outcome of individualised nursing care. Scand J Caring Sci. 2012;26(2):372–80. https://doi.org/10.1111/j.1471-6712.2011.00943.x .
Gaglio B, Shoup JA, Glasgow RE. The RE-AIM framework: a systematic review of use over time. Am J Public Health. 2013;103(6):e38-46. https://doi.org/10.2105/ajph.2013.301299 .
Rye M, Torres EM, Friborg O, Skre I, Aarons GA. The Evidence-based Practice Attitude Scale-36 (EBPAS-36): a brief and pragmatic measure of attitudes to evidence-based practice validated in US and Norwegian samples. Implement Sci. 2017;12(1):44. https://doi.org/10.1186/s13012-017-0573-0 .
Sansoni JE. Health outcomes: an overview from an Australian perspective. 2016;
Sekhon M, Cartwright M, Francis JJ. Acceptability of healthcare interventions: an overview of reviews and development of a theoretical framework. BMC Health Serv Res. 2017;17(1):88. https://doi.org/10.1186/s12913-017-2031-8 .
Weiner BJ, Lewis CC, Stanick C, et al. Psychometric assessment of three newly developed implementation outcome measures. Implement Sci. 2017;12(1):108. https://doi.org/10.1186/s13012-017-0635-3 .
Simoens S. Health economic assessment: a methodological primer. Int J Environ Res Public Health. 2009;6(12):2950–66. https://doi.org/10.3390/ijerph6122950 .
Lorgelly PK, Lawson KD, Fenwick EA, Briggs AH. Outcome measurement in economic evaluations of public health interventions: a role for the capability approach? Int J Environ Res Public Health. 2010;7(5):2274–89. https://doi.org/10.3390/ijerph7052274 .
Williams K, Sansoni J, Morris D, Grootemaat P, Thompson C. Patient-reported outcome measures: literature review. Sydney: Australian Commission on Safety and Quality in Health Care; 2016.
Google Scholar
Zilberberg MD, Shorr AF. Understanding cost-effectiveness. Clin Microbiol Infect. 2010;16(12):1707–12. https://doi.org/10.1111/j.1469-0691.2010.03331.x .
Article CAS PubMed Google Scholar
Feeny DH, Eckstrom E, Whitlock EP, et al. A primer for systematic reviewers on the measurement of functional status and health-related quality of life in older adults [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2013. Available from: https://www.ncbi.nlm.nih.gov/books/NBK169159/ .
Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999;89(9):1322–7. https://doi.org/10.2105/ajph.89.9.1322 .
Article CAS PubMed PubMed Central Google Scholar
Institute of Medicine Committee on Quality of Health Care in America. Crossing the quality chasm: a new health system for the 21st century. National Academies Press (US); 2001.
Higgins JP, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons; 2019.
Book Google Scholar
Williamson PR, Altman DG, Bagley H, et al. The COMET Handbook: version 1.0. Trials. 2017;18(3):280. https://doi.org/10.1186/s13063-017-1978-4 .
Paul CL, Sanson-Fisher R, Douglas HE, Clinton-McHarg T, Williamson A, Barker D. Cutting the research pie: a value-weighting approach to explore perceptions about psychosocial research priorities for adults with haematological cancers. Eur J Cancer Care. 2011;20(3):345–53. https://doi.org/10.1111/j.1365-2354.2010.01188.x .
Article CAS Google Scholar
Fradgley EA, Paul CL, Bryant J, Oldmeadow C. Getting right to the point: identifying Australian outpatients’ priorities and preferences for patient-centred quality improvement in chronic disease care. Int J Qual Health Care. 2016;28(4):470–7. https://doi.org/10.1093/intqhc/mzw049 .
Oliver K, Lorenc T, Tinkler J, Bonell C. Understanding the unintended consequences of public health policies: the views of policymakers and evaluators. BMC Public Health. 2019;19(1):1057. https://doi.org/10.1186/s12889-019-7389-6 .
Sally M, Mark P. Good intentions and received wisdom are not enough. J Epidemiol Community Health. 2000;54(11):802. https://doi.org/10.1136/jech.54.11.802 .
Hoffmann TC, Del Mar C. Clinicians’ expectations of the benefits and harms of treatments, screening, and tests: a systematic review. JAMA Intern Med. 2017;177(3):407–19. https://doi.org/10.1001/jamainternmed.2016.8254 .
Hanoch Y, Rolison J, Freund AM. Reaping the benefits and avoiding the risks: unrealistic optimism in the health domain. Risk Anal. 2019;39(4):792–804. https://doi.org/10.1111/risa.13204 .
Oakley GP Jr, Johnston RB Jr. Balancing benefits and harms in public health prevention programmes mandated by governments. Br Med J. 2004;329(7456):41–3. https://doi.org/10.1136/bmj.329.7456.41 .
Pitt AL, Goldhaber-Fiebert JD, Brandeau ML. Public health interventions with harms and benefits: a graphical framework for evaluating tradeoffs. Med Decis Making. 2020;40(8):978–89. https://doi.org/10.1177/0272989x20960458 .
McDowell M, Rebitschek FG, Gigerenzer G, Wegwarth O. A simple tool for communicating the benefits and harms of health interventions: a guide for creating a fact box. MDM Policy Pract. 2016;1(1):2381468316665365. https://doi.org/10.1177/2381468316665365 .
World Health Organization. Social determinants of health. 2022.
Brownson RC, Kumanyika SK, Kreuter MW, Haire-Joshu D. Implementation science should give higher priority to health equity. Implement Sci. 2021;16(1):28. https://doi.org/10.1186/s13012-021-01097-0 .
Brownson RC, Colditz GA, Proctor EK. Dissemination and implementation research in health: translating science to practice. Oxford University Press; 2017.
Reilly KL, Kennedy S, Porter G, Estabrooks P. Comparing, contrasting, and integrating dissemination and implementation outcomes included in the RE-AIM and implementation outcomes frameworks. Front Public Health. 2020;8:430. https://doi.org/10.3389/fpubh.2020.00430 .
Eisman AB, Kilbourne AM, Dopp AR, Saldana L, Eisenberg D. Economic evaluation in implementation science: making the business case for implementation strategies. Psychiatry Res. 2020;283:112433. https://doi.org/10.1016/j.psychres.2019.06.008 .
Allen P, Pilar M, Walsh-Bailey C, et al. Quantitative measures of health policy implementation determinants and outcomes: a systematic review. Implement Sci. 2020;15(1):47. https://doi.org/10.1186/s13012-020-01007-w .
Whitty JA, Lancsar E, Rixon K, Golenko X, Ratcliffe J. A systematic review of stated preference studies reporting public preferences for healthcare priority setting. Patient. 2014;7(4):365–86. https://doi.org/10.1007/s40271-014-0063-2 .
Smith PG MR, Ross DA, editors, Field trials of health interventions: a toolbox. 3rd edition. Chapter 12, Outcome measures and case definition. 2015.
Wolfenden L, Barnes C, Lane C, et al. Consolidating evidence on the effectiveness of interventions promoting fruit and vegetable consumption: an umbrella review. Int J Behav Nutr Phys Act. 2021;18(1):11. https://doi.org/10.1186/s12966-020-01046-y .
Nathan N, Hall A, McCarthy N, et al. Multi-strategy intervention increases school implementation and maintenance of a mandatory physical activity policy: outcomes of a cluster randomised controlled trial. Br J Sports Med. 2022;56(7):385–93. https://doi.org/10.1136/bjsports-2020-103764 .
Sutherland R, Brown A, Nathan N, et al. A multicomponent mHealth-based intervention (SWAP IT) to decrease the consumption of discretionary foods packed in school lunchboxes: type I effectiveness-implementation hybrid cluster randomized controlled trial. J Med Internet Res. 2021;23(6):e25256. https://doi.org/10.2196/25256 .
Breslin G, Shannon S, Cummings M, Leavey G. An updated systematic review of interventions to increase awareness of mental health and well-being in athletes, coaches, officials and parents. Syst Rev. 2022;11(1):99. https://doi.org/10.1186/s13643-022-01932-5 .
McCrabb S, Lane C, Hall A, et al. Scaling-up evidence-based obesity interventions: a systematic review assessing intervention adaptations and effectiveness and quantifying the scale-up penalty. Obesity Rev. 2019;20(7):964–82. https://doi.org/10.1111/obr.12845 .
Wolfenden L, McCrabb S, Barnes C, et al. Strategies for enhancing the implementation of school-based policies or practices targeting diet, physical activity, obesity, tobacco or alcohol use. Cochrane Database Syst Rev. 2022. https://doi.org/10.1002/14651858.CD011677.pub3 .
Wolfenden L, Barnes C, Jones J, et al. Strategies to improve the implementation of healthy eating, physical activity and obesity prevention policies, practices or programmes within childcare services. Cochrane Database Syst Rev. 2020. https://doi.org/10.1002/14651858.CD011779.pub3 .
Sutherland RL, Jackson JK, Lane C, et al. A systematic review of adaptations and effectiveness of scaled-up nutrition interventions. Nutr Rev. 2022;80(4):962–79. https://doi.org/10.1093/nutrit/nuab096 .
Download references
Acknowledgements
Not applicable.
This study was funded in part by a National Health and Medical Research Council (NHMRC) Centre for Research Excellence – National Centre of Implementation Science (NCOIS) Grant (APP1153479) and a New South Wales (NSW) Cancer Council Program Grant (G1500708). LW is supported by an NHMRC Investigator Grant (G1901360).
Author information
Authors and affiliations.
Faculty of Health and Medicine, School of Medicine and Public Health, University of Newcastle, Newcastle, NSW, 2318, Australia
Luke Wolfenden, Alix Hall, Adrian Bauman, Rebecca Hodder, Emily Webb, Kaitlin Mooney, Serene Yoong, Rachel Sutherland & Sam McCrabb
Hunter New England Population Health, Hunter New England Local Health District, Wallsend, NSW, 2287, Australia
Luke Wolfenden, Alix Hall, Rebecca Hodder, Serene Yoong, Rachel Sutherland & Sam McCrabb
Hunter Medical Research Institute, Newcastle, NSW, 2305, Australia
Prevention Research Collaboration, Charles Perkins Centre, School of Public Health, Faculty of Medicine and Health, The University of Sydney, Sydney, NSW, Australia
Adrian Bauman
The Australian Prevention Partnership Centre, Sydney, NSW, Australia
School of Public Health, University of Sydney, Sydney, NSW, Australia
Andrew Milat
Centre for Epidemiology and Evidence, NSW Ministry of Health, Sydney, Australia
School of Health Sciences, Swinburne University of Technology, Melbourne, VIC, 3122, Australia
Serene Yoong
Global Nutrition and Preventive Health, Institute of Health Transformation, School of Health and Social Development, Deakin University, Burwood, VIC, Australia
You can also search for this author in PubMed Google Scholar
Contributions
LW and SMc led the conception and design of the study, were closely involved in data analysis and interpretation and wrote the manuscript. AH, AB, AM and RH comprised the study advisory committee, reviewed the study’s methods and assisted with survey development. AH was responsible for data analysis. KM and EW assisted with survey development, data collection and preliminary analysis. AH, AB, AM, RH, SY and RS were involved in interpretation and revised the manuscript critically for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Luke Wolfenden .
Ethics declarations
Ethics approval and consent to participate.
Ethics approval was provided by the University of Newcastle Human Research Ethics Committee (H-2014-0070). Implied consent was obtained from participants rather than explicit consent (that is, individuals were not required to expressly provide consent by checking a “I consent box”; rather, undertaking the survey provided implicit consent).
Consent for publication
Competing interests.
The authors declare that they have no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:.
Table S1. Mean point allocations for each of the 17 intervention outcomes overall and by area of expertise (where field of expertise n ≥ 30). Table S2. Mean point allocations for each of the 16 implementation outcomes overall and by area of expertise (where field of expertise n ≥ 30). Table S3. Mean points for implementation outcomes overall and by area of expertise (field of expertise n ≥ 30). Table S4. Sensitivity analysis, participants who selected ‘acceptability’ removed from the analysis, their other rankings remained. Table S5. Sensitivity analysis, participants who selected ‘acceptability’ whole data set removed from the analysis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Wolfenden, L., Hall, A., Bauman, A. et al. Research outcomes informing the selection of public health interventions and strategies to implement them: A cross-sectional survey of Australian policy-maker and practitioner preferences. Health Res Policy Sys 22 , 58 (2024). https://doi.org/10.1186/s12961-024-01144-4
Download citation
Received : 12 July 2023
Accepted : 19 April 2024
Published : 14 May 2024
DOI : https://doi.org/10.1186/s12961-024-01144-4
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Health Research Policy and Systems
ISSN: 1478-4505
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]

Cultural Relativity and Acceptance of Embryonic Stem Cell Research
Article sidebar.

Main Article Content
There is a debate about the ethical implications of using human embryos in stem cell research, which can be influenced by cultural, moral, and social values. This paper argues for an adaptable framework to accommodate diverse cultural and religious perspectives. By using an adaptive ethics model, research protections can reflect various populations and foster growth in stem cell research possibilities.
INTRODUCTION
Stem cell research combines biology, medicine, and technology, promising to alter health care and the understanding of human development. Yet, ethical contention exists because of individuals’ perceptions of using human embryos based on their various cultural, moral, and social values. While these disagreements concerning policy, use, and general acceptance have prompted the development of an international ethics policy, such a uniform approach can overlook the nuanced ethical landscapes between cultures. With diverse viewpoints in public health, a single global policy, especially one reflecting Western ethics or the ethics prevalent in high-income countries, is impractical. This paper argues for a culturally sensitive, adaptable framework for the use of embryonic stem cells. Stem cell policy should accommodate varying ethical viewpoints and promote an effective global dialogue. With an extension of an ethics model that can adapt to various cultures, we recommend localized guidelines that reflect the moral views of the people those guidelines serve.
Stem cells, characterized by their unique ability to differentiate into various cell types, enable the repair or replacement of damaged tissues. Two primary types of stem cells are somatic stem cells (adult stem cells) and embryonic stem cells. Adult stem cells exist in developed tissues and maintain the body’s repair processes. [1] Embryonic stem cells (ESC) are remarkably pluripotent or versatile, making them valuable in research. [2] However, the use of ESCs has sparked ethics debates. Considering the potential of embryonic stem cells, research guidelines are essential. The International Society for Stem Cell Research (ISSCR) provides international stem cell research guidelines. They call for “public conversations touching on the scientific significance as well as the societal and ethical issues raised by ESC research.” [3] The ISSCR also publishes updates about culturing human embryos 14 days post fertilization, suggesting local policies and regulations should continue to evolve as ESC research develops. [4] Like the ISSCR, which calls for local law and policy to adapt to developing stem cell research given cultural acceptance, this paper highlights the importance of local social factors such as religion and culture.
I. Global Cultural Perspective of Embryonic Stem Cells
Views on ESCs vary throughout the world. Some countries readily embrace stem cell research and therapies, while others have stricter regulations due to ethical concerns surrounding embryonic stem cells and when an embryo becomes entitled to moral consideration. The philosophical issue of when the “someone” begins to be a human after fertilization, in the morally relevant sense, [5] impacts when an embryo becomes not just worthy of protection but morally entitled to it. The process of creating embryonic stem cell lines involves the destruction of the embryos for research. [6] Consequently, global engagement in ESC research depends on social-cultural acceptability.
a. US and Rights-Based Cultures
In the United States, attitudes toward stem cell therapies are diverse. The ethics and social approaches, which value individualism, [7] trigger debates regarding the destruction of human embryos, creating a complex regulatory environment. For example, the 1996 Dickey-Wicker Amendment prohibited federal funding for the creation of embryos for research and the destruction of embryos for “more than allowed for research on fetuses in utero.” [8] Following suit, in 2001, the Bush Administration heavily restricted stem cell lines for research. However, the Stem Cell Research Enhancement Act of 2005 was proposed to help develop ESC research but was ultimately vetoed. [9] Under the Obama administration, in 2009, an executive order lifted restrictions allowing for more development in this field. [10] The flux of research capacity and funding parallels the different cultural perceptions of human dignity of the embryo and how it is socially presented within the country’s research culture. [11]
b. Ubuntu and Collective Cultures
African bioethics differs from Western individualism because of the different traditions and values. African traditions, as described by individuals from South Africa and supported by some studies in other African countries, including Ghana and Kenya, follow the African moral philosophies of Ubuntu or Botho and Ukama , which “advocates for a form of wholeness that comes through one’s relationship and connectedness with other people in the society,” [12] making autonomy a socially collective concept. In this context, for the community to act autonomously, individuals would come together to decide what is best for the collective. Thus, stem cell research would require examining the value of the research to society as a whole and the use of the embryos as a collective societal resource. If society views the source as part of the collective whole, and opposes using stem cells, compromising the cultural values to pursue research may cause social detachment and stunt research growth. [13] Based on local culture and moral philosophy, the permissibility of stem cell research depends on how embryo, stem cell, and cell line therapies relate to the community as a whole . Ubuntu is the expression of humanness, with the person’s identity drawn from the “’I am because we are’” value. [14] The decision in a collectivistic culture becomes one born of cultural context, and individual decisions give deference to others in the society.
Consent differs in cultures where thought and moral philosophy are based on a collective paradigm. So, applying Western bioethical concepts is unrealistic. For one, Africa is a diverse continent with many countries with different belief systems, access to health care, and reliance on traditional or Western medicines. Where traditional medicine is the primary treatment, the “’restrictive focus on biomedically-related bioethics’” [is] problematic in African contexts because it neglects bioethical issues raised by traditional systems.” [15] No single approach applies in all areas or contexts. Rather than evaluating the permissibility of ESC research according to Western concepts such as the four principles approach, different ethics approaches should prevail.
Another consideration is the socio-economic standing of countries. In parts of South Africa, researchers have not focused heavily on contributing to the stem cell discourse, either because it is not considered health care or a health science priority or because resources are unavailable. [16] Each country’s priorities differ given different social, political, and economic factors. In South Africa, for instance, areas such as maternal mortality, non-communicable diseases, telemedicine, and the strength of health systems need improvement and require more focus. [17] Stem cell research could benefit the population, but it also could divert resources from basic medical care. Researchers in South Africa adhere to the National Health Act and Medicines Control Act in South Africa and international guidelines; however, the Act is not strictly enforced, and there is no clear legislation for research conduct or ethical guidelines. [18]
Some parts of Africa condemn stem cell research. For example, 98.2 percent of the Tunisian population is Muslim. [19] Tunisia does not permit stem cell research because of moral conflict with a Fatwa. Religion heavily saturates the regulation and direction of research. [20] Stem cell use became permissible for reproductive purposes only recently, with tight restrictions preventing cells from being used in any research other than procedures concerning ART/IVF. Their use is conditioned on consent, and available only to married couples. [21] The community's receptiveness to stem cell research depends on including communitarian African ethics.
c. Asia
Some Asian countries also have a collective model of ethics and decision making. [22] In China, the ethics model promotes a sincere respect for life or human dignity, [23] based on protective medicine. This model, influenced by Traditional Chinese Medicine (TCM), [24] recognizes Qi as the vital energy delivered via the meridians of the body; it connects illness to body systems, the body’s entire constitution, and the universe for a holistic bond of nature, health, and quality of life. [25] Following a protective ethics model, and traditional customs of wholeness, investment in stem cell research is heavily desired for its applications in regenerative therapies, disease modeling, and protective medicines. In a survey of medical students and healthcare practitioners, 30.8 percent considered stem cell research morally unacceptable while 63.5 percent accepted medical research using human embryonic stem cells. Of these individuals, 89.9 percent supported increased funding for stem cell research. [26] The scientific community might not reflect the overall population. From 1997 to 2019, China spent a total of $576 million (USD) on stem cell research at 8,050 stem cell programs, increased published presence from 0.6 percent to 14.01 percent of total global stem cell publications as of 2014, and made significant strides in cell-based therapies for various medical conditions. [27] However, while China has made substantial investments in stem cell research and achieved notable progress in clinical applications, concerns linger regarding ethical oversight and transparency. [28] For example, the China Biosecurity Law, promoted by the National Health Commission and China Hospital Association, attempted to mitigate risks by introducing an institutional review board (IRB) in the regulatory bodies. 5800 IRBs registered with the Chinese Clinical Trial Registry since 2021. [29] However, issues still need to be addressed in implementing effective IRB review and approval procedures.
The substantial government funding and focus on scientific advancement have sometimes overshadowed considerations of regional cultures, ethnic minorities, and individual perspectives, particularly evident during the one-child policy era. As government policy adapts to promote public stability, such as the change from the one-child to the two-child policy, [30] research ethics should also adapt to ensure respect for the values of its represented peoples.
Japan is also relatively supportive of stem cell research and therapies. Japan has a more transparent regulatory framework, allowing for faster approval of regenerative medicine products, which has led to several advanced clinical trials and therapies. [31] South Korea is also actively engaged in stem cell research and has a history of breakthroughs in cloning and embryonic stem cells. [32] However, the field is controversial, and there are issues of scientific integrity. For example, the Korean FDA fast-tracked products for approval, [33] and in another instance, the oocyte source was unclear and possibly violated ethical standards. [34] Trust is important in research, as it builds collaborative foundations between colleagues, trial participant comfort, open-mindedness for complicated and sensitive discussions, and supports regulatory procedures for stakeholders. There is a need to respect the culture’s interest, engagement, and for research and clinical trials to be transparent and have ethical oversight to promote global research discourse and trust.
d. Middle East
Countries in the Middle East have varying degrees of acceptance of or restrictions to policies related to using embryonic stem cells due to cultural and religious influences. Saudi Arabia has made significant contributions to stem cell research, and conducts research based on international guidelines for ethical conduct and under strict adherence to guidelines in accordance with Islamic principles. Specifically, the Saudi government and people require ESC research to adhere to Sharia law. In addition to umbilical and placental stem cells, [35] Saudi Arabia permits the use of embryonic stem cells as long as they come from miscarriages, therapeutic abortions permissible by Sharia law, or are left over from in vitro fertilization and donated to research. [36] Laws and ethical guidelines for stem cell research allow the development of research institutions such as the King Abdullah International Medical Research Center, which has a cord blood bank and a stem cell registry with nearly 10,000 donors. [37] Such volume and acceptance are due to the ethical ‘permissibility’ of the donor sources, which do not conflict with religious pillars. However, some researchers err on the side of caution, choosing not to use embryos or fetal tissue as they feel it is unethical to do so. [38]
Jordan has a positive research ethics culture. [39] However, there is a significant issue of lack of trust in researchers, with 45.23 percent (38.66 percent agreeing and 6.57 percent strongly agreeing) of Jordanians holding a low level of trust in researchers, compared to 81.34 percent of Jordanians agreeing that they feel safe to participate in a research trial. [40] Safety testifies to the feeling of confidence that adequate measures are in place to protect participants from harm, whereas trust in researchers could represent the confidence in researchers to act in the participants’ best interests, adhere to ethical guidelines, provide accurate information, and respect participants’ rights and dignity. One method to improve trust would be to address communication issues relevant to ESC. Legislation surrounding stem cell research has adopted specific language, especially concerning clarification “between ‘stem cells’ and ‘embryonic stem cells’” in translation. [41] Furthermore, legislation “mandates the creation of a national committee… laying out specific regulations for stem-cell banking in accordance with international standards.” [42] This broad regulation opens the door for future global engagement and maintains transparency. However, these regulations may also constrain the influence of research direction, pace, and accessibility of research outcomes.
e. Europe
In the European Union (EU), ethics is also principle-based, but the principles of autonomy, dignity, integrity, and vulnerability are interconnected. [43] As such, the opportunity for cohesion and concessions between individuals’ thoughts and ideals allows for a more adaptable ethics model due to the flexible principles that relate to the human experience The EU has put forth a framework in its Convention for the Protection of Human Rights and Dignity of the Human Being allowing member states to take different approaches. Each European state applies these principles to its specific conventions, leading to or reflecting different acceptance levels of stem cell research. [44]
For example, in Germany, Lebenzusammenhang , or the coherence of life, references integrity in the unity of human culture. Namely, the personal sphere “should not be subject to external intervention.” [45] Stem cell interventions could affect this concept of bodily completeness, leading to heavy restrictions. Under the Grundgesetz, human dignity and the right to life with physical integrity are paramount. [46] The Embryo Protection Act of 1991 made producing cell lines illegal. Cell lines can be imported if approved by the Central Ethics Commission for Stem Cell Research only if they were derived before May 2007. [47] Stem cell research respects the integrity of life for the embryo with heavy specifications and intense oversight. This is vastly different in Finland, where the regulatory bodies find research more permissible in IVF excess, but only up to 14 days after fertilization. [48] Spain’s approach differs still, with a comprehensive regulatory framework. [49] Thus, research regulation can be culture-specific due to variations in applied principles. Diverse cultures call for various approaches to ethical permissibility. [50] Only an adaptive-deliberative model can address the cultural constructions of self and achieve positive, culturally sensitive stem cell research practices. [51]
II. Religious Perspectives on ESC
Embryonic stem cell sources are the main consideration within religious contexts. While individuals may not regard their own religious texts as authoritative or factual, religion can shape their foundations or perspectives.
The Qur'an states:
“And indeed We created man from a quintessence of clay. Then We placed within him a small quantity of nutfa (sperm to fertilize) in a safe place. Then We have fashioned the nutfa into an ‘alaqa (clinging clot or cell cluster), then We developed the ‘alaqa into mudgha (a lump of flesh), and We made mudgha into bones, and clothed the bones with flesh, then We brought it into being as a new creation. So Blessed is Allah, the Best of Creators.” [52]
Many scholars of Islam estimate the time of soul installment, marked by the angel breathing in the soul to bring the individual into creation, as 120 days from conception. [53] Personhood begins at this point, and the value of life would prohibit research or experimentation that could harm the individual. If the fetus is more than 120 days old, the time ensoulment is interpreted to occur according to Islamic law, abortion is no longer permissible. [54] There are a few opposing opinions about early embryos in Islamic traditions. According to some Islamic theologians, there is no ensoulment of the early embryo, which is the source of stem cells for ESC research. [55]
In Buddhism, the stance on stem cell research is not settled. The main tenets, the prohibition against harming or destroying others (ahimsa) and the pursuit of knowledge (prajña) and compassion (karuna), leave Buddhist scholars and communities divided. [56] Some scholars argue stem cell research is in accordance with the Buddhist tenet of seeking knowledge and ending human suffering. Others feel it violates the principle of not harming others. Finding the balance between these two points relies on the karmic burden of Buddhist morality. In trying to prevent ahimsa towards the embryo, Buddhist scholars suggest that to comply with Buddhist tenets, research cannot be done as the embryo has personhood at the moment of conception and would reincarnate immediately, harming the individual's ability to build their karmic burden. [57] On the other hand, the Bodhisattvas, those considered to be on the path to enlightenment or Nirvana, have given organs and flesh to others to help alleviate grieving and to benefit all. [58] Acceptance varies on applied beliefs and interpretations.
Catholicism does not support embryonic stem cell research, as it entails creation or destruction of human embryos. This destruction conflicts with the belief in the sanctity of life. For example, in the Old Testament, Genesis describes humanity as being created in God’s image and multiplying on the Earth, referencing the sacred rights to human conception and the purpose of development and life. In the Ten Commandments, the tenet that one should not kill has numerous interpretations where killing could mean murder or shedding of the sanctity of life, demonstrating the high value of human personhood. In other books, the theological conception of when life begins is interpreted as in utero, [59] highlighting the inviolability of life and its formation in vivo to make a religious point for accepting such research as relatively limited, if at all. [60] The Vatican has released ethical directives to help apply a theological basis to modern-day conflicts. The Magisterium of the Church states that “unless there is a moral certainty of not causing harm,” experimentation on fetuses, fertilized cells, stem cells, or embryos constitutes a crime. [61] Such procedures would not respect the human person who exists at these stages, according to Catholicism. Damages to the embryo are considered gravely immoral and illicit. [62] Although the Catholic Church officially opposes abortion, surveys demonstrate that many Catholic people hold pro-choice views, whether due to the context of conception, stage of pregnancy, threat to the mother’s life, or for other reasons, demonstrating that practicing members can also accept some but not all tenets. [63]
Some major Jewish denominations, such as the Reform, Conservative, and Reconstructionist movements, are open to supporting ESC use or research as long as it is for saving a life. [64] Within Judaism, the Talmud, or study, gives personhood to the child at birth and emphasizes that life does not begin at conception: [65]
“If she is found pregnant, until the fortieth day it is mere fluid,” [66]
Whereas most religions prioritize the status of human embryos, the Halakah (Jewish religious law) states that to save one life, most other religious laws can be ignored because it is in pursuit of preservation. [67] Stem cell research is accepted due to application of these religious laws.
We recognize that all religions contain subsets and sects. The variety of environmental and cultural differences within religious groups requires further analysis to respect the flexibility of religious thoughts and practices. We make no presumptions that all cultures require notions of autonomy or morality as under the common morality theory , which asserts a set of universal moral norms that all individuals share provides moral reasoning and guides ethical decisions. [68] We only wish to show that the interaction with morality varies between cultures and countries.
III. A Flexible Ethical Approach
The plurality of different moral approaches described above demonstrates that there can be no universally acceptable uniform law for ESC on a global scale. Instead of developing one standard, flexible ethical applications must be continued. We recommend local guidelines that incorporate important cultural and ethical priorities.
While the Declaration of Helsinki is more relevant to people in clinical trials receiving ESC products, in keeping with the tradition of protections for research subjects, consent of the donor is an ethical requirement for ESC donation in many jurisdictions including the US, Canada, and Europe. [69] The Declaration of Helsinki provides a reference point for regulatory standards and could potentially be used as a universal baseline for obtaining consent prior to gamete or embryo donation.
For instance, in Columbia University’s egg donor program for stem cell research, donors followed standard screening protocols and “underwent counseling sessions that included information as to the purpose of oocyte donation for research, what the oocytes would be used for, the risks and benefits of donation, and process of oocyte stimulation” to ensure transparency for consent. [70] The program helped advance stem cell research and provided clear and safe research methods with paid participants. Though paid participation or covering costs of incidental expenses may not be socially acceptable in every culture or context, [71] and creating embryos for ESC research is illegal in many jurisdictions, Columbia’s program was effective because of the clear and honest communications with donors, IRBs, and related stakeholders. This example demonstrates that cultural acceptance of scientific research and of the idea that an egg or embryo does not have personhood is likely behind societal acceptance of donating eggs for ESC research. As noted, many countries do not permit the creation of embryos for research.
Proper communication and education regarding the process and purpose of stem cell research may bolster comprehension and garner more acceptance. “Given the sensitive subject material, a complete consent process can support voluntary participation through trust, understanding, and ethical norms from the cultures and morals participants value. This can be hard for researchers entering countries of different socioeconomic stability, with different languages and different societal values. [72]
An adequate moral foundation in medical ethics is derived from the cultural and religious basis that informs knowledge and actions. [73] Understanding local cultural and religious values and their impact on research could help researchers develop humility and promote inclusion.
IV. Concerns
Some may argue that if researchers all adhere to one ethics standard, protection will be satisfied across all borders, and the global public will trust researchers. However, defining what needs to be protected and how to define such research standards is very specific to the people to which standards are applied. We suggest that applying one uniform guide cannot accurately protect each individual because we all possess our own perceptions and interpretations of social values. [74] Therefore, the issue of not adjusting to the moral pluralism between peoples in applying one standard of ethics can be resolved by building out ethics models that can be adapted to different cultures and religions.
Other concerns include medical tourism, which may promote health inequities. [75] Some countries may develop and approve products derived from ESC research before others, compromising research ethics or drug approval processes. There are also concerns about the sale of unauthorized stem cell treatments, for example, those without FDA approval in the United States. Countries with robust research infrastructures may be tempted to attract medical tourists, and some customers will have false hopes based on aggressive publicity of unproven treatments. [76]
For example, in China, stem cell clinics can market to foreign clients who are not protected under the regulatory regimes. Companies employ a marketing strategy of “ethically friendly” therapies. Specifically, in the case of Beike, China’s leading stem cell tourism company and sprouting network, ethical oversight of administrators or health bureaus at one site has “the unintended consequence of shifting questionable activities to another node in Beike's diffuse network.” [77] In contrast, Jordan is aware of stem cell research’s potential abuse and its own status as a “health-care hub.” Jordan’s expanded regulations include preserving the interests of individuals in clinical trials and banning private companies from ESC research to preserve transparency and the integrity of research practices. [78]
The social priorities of the community are also a concern. The ISSCR explicitly states that guidelines “should be periodically revised to accommodate scientific advances, new challenges, and evolving social priorities.” [79] The adaptable ethics model extends this consideration further by addressing whether research is warranted given the varying degrees of socioeconomic conditions, political stability, and healthcare accessibilities and limitations. An ethical approach would require discussion about resource allocation and appropriate distribution of funds. [80]
While some religions emphasize the sanctity of life from conception, which may lead to public opposition to ESC research, others encourage ESC research due to its potential for healing and alleviating human pain. Many countries have special regulations that balance local views on embryonic personhood, the benefits of research as individual or societal goods, and the protection of human research subjects. To foster understanding and constructive dialogue, global policy frameworks should prioritize the protection of universal human rights, transparency, and informed consent. In addition to these foundational global policies, we recommend tailoring local guidelines to reflect the diverse cultural and religious perspectives of the populations they govern. Ethics models should be adapted to local populations to effectively establish research protections, growth, and possibilities of stem cell research.
For example, in countries with strong beliefs in the moral sanctity of embryos or heavy religious restrictions, an adaptive model can allow for discussion instead of immediate rejection. In countries with limited individual rights and voice in science policy, an adaptive model ensures cultural, moral, and religious views are taken into consideration, thereby building social inclusion. While this ethical consideration by the government may not give a complete voice to every individual, it will help balance policies and maintain the diverse perspectives of those it affects. Embracing an adaptive ethics model of ESC research promotes open-minded dialogue and respect for the importance of human belief and tradition. By actively engaging with cultural and religious values, researchers can better handle disagreements and promote ethical research practices that benefit each society.
This brief exploration of the religious and cultural differences that impact ESC research reveals the nuances of relative ethics and highlights a need for local policymakers to apply a more intense adaptive model.
[1] Poliwoda, S., Noor, N., Downs, E., Schaaf, A., Cantwell, A., Ganti, L., Kaye, A. D., Mosel, L. I., Carroll, C. B., Viswanath, O., & Urits, I. (2022). Stem cells: a comprehensive review of origins and emerging clinical roles in medical practice. Orthopedic reviews , 14 (3), 37498. https://doi.org/10.52965/001c.37498
[2] Poliwoda, S., Noor, N., Downs, E., Schaaf, A., Cantwell, A., Ganti, L., Kaye, A. D., Mosel, L. I., Carroll, C. B., Viswanath, O., & Urits, I. (2022). Stem cells: a comprehensive review of origins and emerging clinical roles in medical practice. Orthopedic reviews , 14 (3), 37498. https://doi.org/10.52965/001c.37498
[3] International Society for Stem Cell Research. (2023). Laboratory-based human embryonic stem cell research, embryo research, and related research activities . International Society for Stem Cell Research. https://www.isscr.org/guidelines/blog-post-title-one-ed2td-6fcdk ; Kimmelman, J., Hyun, I., Benvenisty, N. et al. Policy: Global standards for stem-cell research. Nature 533 , 311–313 (2016). https://doi.org/10.1038/533311a
[4] International Society for Stem Cell Research. (2023). Laboratory-based human embryonic stem cell research, embryo research, and related research activities . International Society for Stem Cell Research. https://www.isscr.org/guidelines/blog-post-title-one-ed2td-6fcdk
[5] Concerning the moral philosophies of stem cell research, our paper does not posit a personal moral stance nor delve into the “when” of human life begins. To read further about the philosophical debate, consider the following sources:
Sandel M. J. (2004). Embryo ethics--the moral logic of stem-cell research. The New England journal of medicine , 351 (3), 207–209. https://doi.org/10.1056/NEJMp048145 ; George, R. P., & Lee, P. (2020, September 26). Acorns and Embryos . The New Atlantis. https://www.thenewatlantis.com/publications/acorns-and-embryos ; Sagan, A., & Singer, P. (2007). The moral status of stem cells. Metaphilosophy , 38 (2/3), 264–284. http://www.jstor.org/stable/24439776 ; McHugh P. R. (2004). Zygote and "clonote"--the ethical use of embryonic stem cells. The New England journal of medicine , 351 (3), 209–211. https://doi.org/10.1056/NEJMp048147 ; Kurjak, A., & Tripalo, A. (2004). The facts and doubts about beginning of the human life and personality. Bosnian journal of basic medical sciences , 4 (1), 5–14. https://doi.org/10.17305/bjbms.2004.3453
[6] Vazin, T., & Freed, W. J. (2010). Human embryonic stem cells: derivation, culture, and differentiation: a review. Restorative neurology and neuroscience , 28 (4), 589–603. https://doi.org/10.3233/RNN-2010-0543
[7] Socially, at its core, the Western approach to ethics is widely principle-based, autonomy being one of the key factors to ensure a fundamental respect for persons within research. For information regarding autonomy in research, see: Department of Health, Education, and Welfare, & National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research (1978). The Belmont Report. Ethical principles and guidelines for the protection of human subjects of research.; For a more in-depth review of autonomy within the US, see: Beauchamp, T. L., & Childress, J. F. (1994). Principles of Biomedical Ethics . Oxford University Press.
[8] Sherley v. Sebelius , 644 F.3d 388 (D.C. Cir. 2011), citing 45 C.F.R. 46.204(b) and [42 U.S.C. § 289g(b)]. https://www.cadc.uscourts.gov/internet/opinions.nsf/6c690438a9b43dd685257a64004ebf99/$file/11-5241-1391178.pdf
[9] Stem Cell Research Enhancement Act of 2005, H. R. 810, 109 th Cong. (2001). https://www.govtrack.us/congress/bills/109/hr810/text ; Bush, G. W. (2006, July 19). Message to the House of Representatives . National Archives and Records Administration. https://georgewbush-whitehouse.archives.gov/news/releases/2006/07/20060719-5.html
[10] National Archives and Records Administration. (2009, March 9). Executive order 13505 -- removing barriers to responsible scientific research involving human stem cells . National Archives and Records Administration. https://obamawhitehouse.archives.gov/the-press-office/removing-barriers-responsible-scientific-research-involving-human-stem-cells
[11] Hurlbut, W. B. (2006). Science, Religion, and the Politics of Stem Cells. Social Research , 73 (3), 819–834. http://www.jstor.org/stable/40971854
[12] Akpa-Inyang, Francis & Chima, Sylvester. (2021). South African traditional values and beliefs regarding informed consent and limitations of the principle of respect for autonomy in African communities: a cross-cultural qualitative study. BMC Medical Ethics . 22. 10.1186/s12910-021-00678-4.
[13] Source for further reading: Tangwa G. B. (2007). Moral status of embryonic stem cells: perspective of an African villager. Bioethics , 21(8), 449–457. https://doi.org/10.1111/j.1467-8519.2007.00582.x , see also Mnisi, F. M. (2020). An African analysis based on ethics of Ubuntu - are human embryonic stem cell patents morally justifiable? African Insight , 49 (4).
[14] Jecker, N. S., & Atuire, C. (2021). Bioethics in Africa: A contextually enlightened analysis of three cases. Developing World Bioethics , 22 (2), 112–122. https://doi.org/10.1111/dewb.12324
[15] Jecker, N. S., & Atuire, C. (2021). Bioethics in Africa: A contextually enlightened analysis of three cases. Developing World Bioethics, 22(2), 112–122. https://doi.org/10.1111/dewb.12324
[16] Jackson, C.S., Pepper, M.S. Opportunities and barriers to establishing a cell therapy programme in South Africa. Stem Cell Res Ther 4 , 54 (2013). https://doi.org/10.1186/scrt204 ; Pew Research Center. (2014, May 1). Public health a major priority in African nations . Pew Research Center’s Global Attitudes Project. https://www.pewresearch.org/global/2014/05/01/public-health-a-major-priority-in-african-nations/
[17] Department of Health Republic of South Africa. (2021). Health Research Priorities (revised) for South Africa 2021-2024 . National Health Research Strategy. https://www.health.gov.za/wp-content/uploads/2022/05/National-Health-Research-Priorities-2021-2024.pdf
[18] Oosthuizen, H. (2013). Legal and Ethical Issues in Stem Cell Research in South Africa. In: Beran, R. (eds) Legal and Forensic Medicine. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-32338-6_80 , see also: Gaobotse G (2018) Stem Cell Research in Africa: Legislation and Challenges. J Regen Med 7:1. doi: 10.4172/2325-9620.1000142
[19] United States Bureau of Citizenship and Immigration Services. (1998). Tunisia: Information on the status of Christian conversions in Tunisia . UNHCR Web Archive. https://webarchive.archive.unhcr.org/20230522142618/https://www.refworld.org/docid/3df0be9a2.html
[20] Gaobotse, G. (2018) Stem Cell Research in Africa: Legislation and Challenges. J Regen Med 7:1. doi: 10.4172/2325-9620.1000142
[21] Kooli, C. Review of assisted reproduction techniques, laws, and regulations in Muslim countries. Middle East Fertil Soc J 24 , 8 (2020). https://doi.org/10.1186/s43043-019-0011-0 ; Gaobotse, G. (2018) Stem Cell Research in Africa: Legislation and Challenges. J Regen Med 7:1. doi: 10.4172/2325-9620.1000142
[22] Pang M. C. (1999). Protective truthfulness: the Chinese way of safeguarding patients in informed treatment decisions. Journal of medical ethics , 25(3), 247–253. https://doi.org/10.1136/jme.25.3.247
[23] Wang, L., Wang, F., & Zhang, W. (2021). Bioethics in China’s biosecurity law: Forms, effects, and unsettled issues. Journal of law and the biosciences , 8(1). https://doi.org/10.1093/jlb/lsab019 https://academic.oup.com/jlb/article/8/1/lsab019/6299199
[24] Wang, Y., Xue, Y., & Guo, H. D. (2022). Intervention effects of traditional Chinese medicine on stem cell therapy of myocardial infarction. Frontiers in pharmacology , 13 , 1013740. https://doi.org/10.3389/fphar.2022.1013740
[25] Li, X.-T., & Zhao, J. (2012). Chapter 4: An Approach to the Nature of Qi in TCM- Qi and Bioenergy. In Recent Advances in Theories and Practice of Chinese Medicine (p. 79). InTech.
[26] Luo, D., Xu, Z., Wang, Z., & Ran, W. (2021). China's Stem Cell Research and Knowledge Levels of Medical Practitioners and Students. Stem cells international , 2021 , 6667743. https://doi.org/10.1155/2021/6667743
[27] Luo, D., Xu, Z., Wang, Z., & Ran, W. (2021). China's Stem Cell Research and Knowledge Levels of Medical Practitioners and Students. Stem cells international , 2021 , 6667743. https://doi.org/10.1155/2021/6667743
[28] Zhang, J. Y. (2017). Lost in translation? accountability and governance of Clinical Stem Cell Research in China. Regenerative Medicine , 12 (6), 647–656. https://doi.org/10.2217/rme-2017-0035
[29] Wang, L., Wang, F., & Zhang, W. (2021). Bioethics in China’s biosecurity law: Forms, effects, and unsettled issues. Journal of law and the biosciences , 8(1). https://doi.org/10.1093/jlb/lsab019 https://academic.oup.com/jlb/article/8/1/lsab019/6299199
[30] Chen, H., Wei, T., Wang, H. et al. Association of China’s two-child policy with changes in number of births and birth defects rate, 2008–2017. BMC Public Health 22 , 434 (2022). https://doi.org/10.1186/s12889-022-12839-0
[31] Azuma, K. Regulatory Landscape of Regenerative Medicine in Japan. Curr Stem Cell Rep 1 , 118–128 (2015). https://doi.org/10.1007/s40778-015-0012-6
[32] Harris, R. (2005, May 19). Researchers Report Advance in Stem Cell Production . NPR. https://www.npr.org/2005/05/19/4658967/researchers-report-advance-in-stem-cell-production
[33] Park, S. (2012). South Korea steps up stem-cell work. Nature . https://doi.org/10.1038/nature.2012.10565
[34] Resnik, D. B., Shamoo, A. E., & Krimsky, S. (2006). Fraudulent human embryonic stem cell research in South Korea: lessons learned. Accountability in research , 13 (1), 101–109. https://doi.org/10.1080/08989620600634193 .
[35] Alahmad, G., Aljohani, S., & Najjar, M. F. (2020). Ethical challenges regarding the use of stem cells: interviews with researchers from Saudi Arabia. BMC medical ethics, 21(1), 35. https://doi.org/10.1186/s12910-020-00482-6
[36] Association for the Advancement of Blood and Biotherapies. https://www.aabb.org/regulatory-and-advocacy/regulatory-affairs/regulatory-for-cellular-therapies/international-competent-authorities/saudi-arabia
[37] Alahmad, G., Aljohani, S., & Najjar, M. F. (2020). Ethical challenges regarding the use of stem cells: Interviews with researchers from Saudi Arabia. BMC medical ethics , 21 (1), 35. https://doi.org/10.1186/s12910-020-00482-6
[38] Alahmad, G., Aljohani, S., & Najjar, M. F. (2020). Ethical challenges regarding the use of stem cells: Interviews with researchers from Saudi Arabia. BMC medical ethics , 21(1), 35. https://doi.org/10.1186/s12910-020-00482-6
Culturally, autonomy practices follow a relational autonomy approach based on a paternalistic deontological health care model. The adherence to strict international research policies and religious pillars within the regulatory environment is a great foundation for research ethics. However, there is a need to develop locally targeted ethics approaches for research (as called for in Alahmad, G., Aljohani, S., & Najjar, M. F. (2020). Ethical challenges regarding the use of stem cells: interviews with researchers from Saudi Arabia. BMC medical ethics, 21(1), 35. https://doi.org/10.1186/s12910-020-00482-6), this decision-making approach may help advise a research decision model. For more on the clinical cultural autonomy approaches, see: Alabdullah, Y. Y., Alzaid, E., Alsaad, S., Alamri, T., Alolayan, S. W., Bah, S., & Aljoudi, A. S. (2022). Autonomy and paternalism in Shared decision‐making in a Saudi Arabian tertiary hospital: A cross‐sectional study. Developing World Bioethics , 23 (3), 260–268. https://doi.org/10.1111/dewb.12355 ; Bukhari, A. A. (2017). Universal Principles of Bioethics and Patient Rights in Saudi Arabia (Doctoral dissertation, Duquesne University). https://dsc.duq.edu/etd/124; Ladha, S., Nakshawani, S. A., Alzaidy, A., & Tarab, B. (2023, October 26). Islam and Bioethics: What We All Need to Know . Columbia University School of Professional Studies. https://sps.columbia.edu/events/islam-and-bioethics-what-we-all-need-know
[39] Ababneh, M. A., Al-Azzam, S. I., Alzoubi, K., Rababa’h, A., & Al Demour, S. (2021). Understanding and attitudes of the Jordanian public about clinical research ethics. Research Ethics , 17 (2), 228-241. https://doi.org/10.1177/1747016120966779
[40] Ababneh, M. A., Al-Azzam, S. I., Alzoubi, K., Rababa’h, A., & Al Demour, S. (2021). Understanding and attitudes of the Jordanian public about clinical research ethics. Research Ethics , 17 (2), 228-241. https://doi.org/10.1177/1747016120966779
[41] Dajani, R. (2014). Jordan’s stem-cell law can guide the Middle East. Nature 510, 189. https://doi.org/10.1038/510189a
[42] Dajani, R. (2014). Jordan’s stem-cell law can guide the Middle East. Nature 510, 189. https://doi.org/10.1038/510189a
[43] The EU’s definition of autonomy relates to the capacity for creating ideas, moral insight, decisions, and actions without constraint, personal responsibility, and informed consent. However, the EU views autonomy as not completely able to protect individuals and depends on other principles, such as dignity, which “expresses the intrinsic worth and fundamental equality of all human beings.” Rendtorff, J.D., Kemp, P. (2019). Four Ethical Principles in European Bioethics and Biolaw: Autonomy, Dignity, Integrity and Vulnerability. In: Valdés, E., Lecaros, J. (eds) Biolaw and Policy in the Twenty-First Century. International Library of Ethics, Law, and the New Medicine, vol 78. Springer, Cham. https://doi.org/10.1007/978-3-030-05903-3_3
[44] Council of Europe. Convention for the protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine: Convention on Human Rights and Biomedicine (ETS No. 164) https://www.coe.int/en/web/conventions/full-list?module=treaty-detail&treatynum=164 (forbidding the creation of embryos for research purposes only, and suggests embryos in vitro have protections.); Also see Drabiak-Syed B. K. (2013). New President, New Human Embryonic Stem Cell Research Policy: Comparative International Perspectives and Embryonic Stem Cell Research Laws in France. Biotechnology Law Report , 32 (6), 349–356. https://doi.org/10.1089/blr.2013.9865
[45] Rendtorff, J.D., Kemp, P. (2019). Four Ethical Principles in European Bioethics and Biolaw: Autonomy, Dignity, Integrity and Vulnerability. In: Valdés, E., Lecaros, J. (eds) Biolaw and Policy in the Twenty-First Century. International Library of Ethics, Law, and the New Medicine, vol 78. Springer, Cham. https://doi.org/10.1007/978-3-030-05903-3_3
[46] Tomuschat, C., Currie, D. P., Kommers, D. P., & Kerr, R. (Trans.). (1949, May 23). Basic law for the Federal Republic of Germany. https://www.btg-bestellservice.de/pdf/80201000.pdf
[47] Regulation of Stem Cell Research in Germany . Eurostemcell. (2017, April 26). https://www.eurostemcell.org/regulation-stem-cell-research-germany
[48] Regulation of Stem Cell Research in Finland . Eurostemcell. (2017, April 26). https://www.eurostemcell.org/regulation-stem-cell-research-finland
[49] Regulation of Stem Cell Research in Spain . Eurostemcell. (2017, April 26). https://www.eurostemcell.org/regulation-stem-cell-research-spain
[50] Some sources to consider regarding ethics models or regulatory oversights of other cultures not covered:
Kara MA. Applicability of the principle of respect for autonomy: the perspective of Turkey. J Med Ethics. 2007 Nov;33(11):627-30. doi: 10.1136/jme.2006.017400. PMID: 17971462; PMCID: PMC2598110.
Ugarte, O. N., & Acioly, M. A. (2014). The principle of autonomy in Brazil: one needs to discuss it ... Revista do Colegio Brasileiro de Cirurgioes , 41 (5), 374–377. https://doi.org/10.1590/0100-69912014005013
Bharadwaj, A., & Glasner, P. E. (2012). Local cells, global science: The rise of embryonic stem cell research in India . Routledge.
For further research on specific European countries regarding ethical and regulatory framework, we recommend this database: Regulation of Stem Cell Research in Europe . Eurostemcell. (2017, April 26). https://www.eurostemcell.org/regulation-stem-cell-research-europe
[51] Klitzman, R. (2006). Complications of culture in obtaining informed consent. The American Journal of Bioethics, 6(1), 20–21. https://doi.org/10.1080/15265160500394671 see also: Ekmekci, P. E., & Arda, B. (2017). Interculturalism and Informed Consent: Respecting Cultural Differences without Breaching Human Rights. Cultura (Iasi, Romania) , 14 (2), 159–172.; For why trust is important in research, see also: Gray, B., Hilder, J., Macdonald, L., Tester, R., Dowell, A., & Stubbe, M. (2017). Are research ethics guidelines culturally competent? Research Ethics , 13 (1), 23-41. https://doi.org/10.1177/1747016116650235
[52] The Qur'an (M. Khattab, Trans.). (1965). Al-Mu’minun, 23: 12-14. https://quran.com/23
[53] Lenfest, Y. (2017, December 8). Islam and the beginning of human life . Bill of Health. https://blog.petrieflom.law.harvard.edu/2017/12/08/islam-and-the-beginning-of-human-life/
[54] Aksoy, S. (2005). Making regulations and drawing up legislation in Islamic countries under conditions of uncertainty, with special reference to embryonic stem cell research. Journal of Medical Ethics , 31: 399-403.; see also: Mahmoud, Azza. "Islamic Bioethics: National Regulations and Guidelines of Human Stem Cell Research in the Muslim World." Master's thesis, Chapman University, 2022. https://doi.org/10.36837/ chapman.000386
[55] Rashid, R. (2022). When does Ensoulment occur in the Human Foetus. Journal of the British Islamic Medical Association , 12 (4). ISSN 2634 8071. https://www.jbima.com/wp-content/uploads/2023/01/2-Ethics-3_-Ensoulment_Rafaqat.pdf.
[56] Sivaraman, M. & Noor, S. (2017). Ethics of embryonic stem cell research according to Buddhist, Hindu, Catholic, and Islamic religions: perspective from Malaysia. Asian Biomedicine,8(1) 43-52. https://doi.org/10.5372/1905-7415.0801.260
[57] Jafari, M., Elahi, F., Ozyurt, S. & Wrigley, T. (2007). 4. Religious Perspectives on Embryonic Stem Cell Research. In K. Monroe, R. Miller & J. Tobis (Ed.), Fundamentals of the Stem Cell Debate: The Scientific, Religious, Ethical, and Political Issues (pp. 79-94). Berkeley: University of California Press. https://escholarship.org/content/qt9rj0k7s3/qt9rj0k7s3_noSplash_f9aca2e02c3777c7fb76ea768ba458f0.pdf https://doi.org/10.1525/9780520940994-005
[58] Lecso, P. A. (1991). The Bodhisattva Ideal and Organ Transplantation. Journal of Religion and Health , 30 (1), 35–41. http://www.jstor.org/stable/27510629 ; Bodhisattva, S. (n.d.). The Key of Becoming a Bodhisattva . A Guide to the Bodhisattva Way of Life. http://www.buddhism.org/Sutras/2/BodhisattvaWay.htm
[59] There is no explicit religious reference to when life begins or how to conduct research that interacts with the concept of life. However, these are relevant verses pertaining to how the fetus is viewed. (( King James Bible . (1999). Oxford University Press. (original work published 1769))
Jerimiah 1: 5 “Before I formed thee in the belly I knew thee; and before thou camest forth out of the womb I sanctified thee…”
In prophet Jerimiah’s insight, God set him apart as a person known before childbirth, a theme carried within the Psalm of David.
Psalm 139: 13-14 “…Thou hast covered me in my mother's womb. I will praise thee; for I am fearfully and wonderfully made…”
These verses demonstrate David’s respect for God as an entity that would know of all man’s thoughts and doings even before birth.
[60] It should be noted that abortion is not supported as well.
[61] The Vatican. (1987, February 22). Instruction on Respect for Human Life in Its Origin and on the Dignity of Procreation Replies to Certain Questions of the Day . Congregation For the Doctrine of the Faith. https://www.vatican.va/roman_curia/congregations/cfaith/documents/rc_con_cfaith_doc_19870222_respect-for-human-life_en.html
[62] The Vatican. (2000, August 25). Declaration On the Production and the Scientific and Therapeutic Use of Human Embryonic Stem Cells . Pontifical Academy for Life. https://www.vatican.va/roman_curia/pontifical_academies/acdlife/documents/rc_pa_acdlife_doc_20000824_cellule-staminali_en.html ; Ohara, N. (2003). Ethical Consideration of Experimentation Using Living Human Embryos: The Catholic Church’s Position on Human Embryonic Stem Cell Research and Human Cloning. Department of Obstetrics and Gynecology . Retrieved from https://article.imrpress.com/journal/CEOG/30/2-3/pii/2003018/77-81.pdf.
[63] Smith, G. A. (2022, May 23). Like Americans overall, Catholics vary in their abortion views, with regular mass attenders most opposed . Pew Research Center. https://www.pewresearch.org/short-reads/2022/05/23/like-americans-overall-catholics-vary-in-their-abortion-views-with-regular-mass-attenders-most-opposed/
[64] Rosner, F., & Reichman, E. (2002). Embryonic stem cell research in Jewish law. Journal of halacha and contemporary society , (43), 49–68.; Jafari, M., Elahi, F., Ozyurt, S. & Wrigley, T. (2007). 4. Religious Perspectives on Embryonic Stem Cell Research. In K. Monroe, R. Miller & J. Tobis (Ed.), Fundamentals of the Stem Cell Debate: The Scientific, Religious, Ethical, and Political Issues (pp. 79-94). Berkeley: University of California Press. https://escholarship.org/content/qt9rj0k7s3/qt9rj0k7s3_noSplash_f9aca2e02c3777c7fb76ea768ba458f0.pdf https://doi.org/10.1525/9780520940994-005
[65] Schenker J. G. (2008). The beginning of human life: status of embryo. Perspectives in Halakha (Jewish Religious Law). Journal of assisted reproduction and genetics , 25 (6), 271–276. https://doi.org/10.1007/s10815-008-9221-6
[66] Ruttenberg, D. (2020, May 5). The Torah of Abortion Justice (annotated source sheet) . Sefaria. https://www.sefaria.org/sheets/234926.7?lang=bi&with=all&lang2=en
[67] Jafari, M., Elahi, F., Ozyurt, S. & Wrigley, T. (2007). 4. Religious Perspectives on Embryonic Stem Cell Research. In K. Monroe, R. Miller & J. Tobis (Ed.), Fundamentals of the Stem Cell Debate: The Scientific, Religious, Ethical, and Political Issues (pp. 79-94). Berkeley: University of California Press. https://escholarship.org/content/qt9rj0k7s3/qt9rj0k7s3_noSplash_f9aca2e02c3777c7fb76ea768ba458f0.pdf https://doi.org/10.1525/9780520940994-005
[68] Gert, B. (2007). Common morality: Deciding what to do . Oxford Univ. Press.
[69] World Medical Association (2013). World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA , 310(20), 2191–2194. https://doi.org/10.1001/jama.2013.281053 Declaration of Helsinki – WMA – The World Medical Association .; see also: National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. (1979). The Belmont report: Ethical principles and guidelines for the protection of human subjects of research . U.S. Department of Health and Human Services. https://www.hhs.gov/ohrp/regulations-and-policy/belmont-report/read-the-belmont-report/index.html
[70] Zakarin Safier, L., Gumer, A., Kline, M., Egli, D., & Sauer, M. V. (2018). Compensating human subjects providing oocytes for stem cell research: 9-year experience and outcomes. Journal of assisted reproduction and genetics , 35 (7), 1219–1225. https://doi.org/10.1007/s10815-018-1171-z https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6063839/ see also: Riordan, N. H., & Paz Rodríguez, J. (2021). Addressing concerns regarding associated costs, transparency, and integrity of research in recent stem cell trial. Stem Cells Translational Medicine , 10 (12), 1715–1716. https://doi.org/10.1002/sctm.21-0234
[71] Klitzman, R., & Sauer, M. V. (2009). Payment of egg donors in stem cell research in the USA. Reproductive biomedicine online , 18 (5), 603–608. https://doi.org/10.1016/s1472-6483(10)60002-8
[72] Krosin, M. T., Klitzman, R., Levin, B., Cheng, J., & Ranney, M. L. (2006). Problems in comprehension of informed consent in rural and peri-urban Mali, West Africa. Clinical trials (London, England) , 3 (3), 306–313. https://doi.org/10.1191/1740774506cn150oa
[73] Veatch, Robert M. Hippocratic, Religious, and Secular Medical Ethics: The Points of Conflict . Georgetown University Press, 2012.
[74] Msoroka, M. S., & Amundsen, D. (2018). One size fits not quite all: Universal research ethics with diversity. Research Ethics , 14 (3), 1-17. https://doi.org/10.1177/1747016117739939
[75] Pirzada, N. (2022). The Expansion of Turkey’s Medical Tourism Industry. Voices in Bioethics , 8 . https://doi.org/10.52214/vib.v8i.9894
[76] Stem Cell Tourism: False Hope for Real Money . Harvard Stem Cell Institute (HSCI). (2023). https://hsci.harvard.edu/stem-cell-tourism , See also: Bissassar, M. (2017). Transnational Stem Cell Tourism: An ethical analysis. Voices in Bioethics , 3 . https://doi.org/10.7916/vib.v3i.6027
[77] Song, P. (2011) The proliferation of stem cell therapies in post-Mao China: problematizing ethical regulation, New Genetics and Society , 30:2, 141-153, DOI: 10.1080/14636778.2011.574375
[78] Dajani, R. (2014). Jordan’s stem-cell law can guide the Middle East. Nature 510, 189. https://doi.org/10.1038/510189a
[79] International Society for Stem Cell Research. (2024). Standards in stem cell research . International Society for Stem Cell Research. https://www.isscr.org/guidelines/5-standards-in-stem-cell-research
[80] Benjamin, R. (2013). People’s science bodies and rights on the Stem Cell Frontier . Stanford University Press.
Mifrah Hayath
SM Candidate Harvard Medical School, MS Biotechnology Johns Hopkins University
Olivia Bowers
MS Bioethics Columbia University (Disclosure: affiliated with Voices in Bioethics)
Article Details

This work is licensed under a Creative Commons Attribution 4.0 International License .
- The main difference between research and...
The main difference between research and non-research is
The main difference between research and non-research is 1). the type of skills we use to discover something. 2). the utilization of acceptable scientific methodology to solve problems to create new knowledge. 3). the quantitative and qualitative methods that are to be used. 4). all the above.
UGC NET Paper 1 Best Book
UGC NET Facebook Page
the utilization of acceptable scientific methodology to solve problems to create new knowledge.
Join Telegram Group
Other Questions
1. Data analysis can be in
2. which of the following is the purpose of reference
3. Which one of the following is a disadvantage of Randomization?
4. On the basis of the nature of variable, the types of survey method are
5. which of the following study does not need hypotheses
6. Alteration in performance due to being aware that one is participating in a study is known as ........
7. People who are available, volunteer, or can be easily recruited are used in the sampling method called ........
8. What is the problem(s) with this set of response categories to the question"What is your current age?" 1-5 5-10 10-20 20-30 30-40
9. Which is an example of a properly written research question?
10. Who said that there are four criteria sources for identifying the problem of educational research?
General Knowledge Questions
Political Science
Enviornmental Science
Books & Authors
Computer Basics
Financial Awareness
International Organisations
Famous Personalities
English Language and Comprehension
Spoting Errors
Sentence Improvement
Fill In the Blanks
Idioms and Phrases
Voice (Active/ Passive)
Naration (Direct/ Indirect)
Reading Comprehension
Quantitative Aptitude
Mensuration
Simplification
Profit & Loss
Trigonometry
Ratio & Proportion
Time & Work
Simple & Compound Interest
Number System
Time & Distance
Surds and Indices
Mixture & Alligation
Co-Ordinate Geometry
Pipe & Cistern
Probability
Boat & Streams
Problem on Age
Permutation & Combination
Problem on Trains
ExamCompetition 2015-2021
Social Cognitive and Addiction Neuroscience Lab at the University of Iowa
Research in the scanlab.

Research projects in the UIOWA Social Cognitive and Addiction Neuroscience Lab generally focus on one of the following areas:
The role of cognitive control in social behavior
Effects of alcohol on cognitive control
Individual differences in neurobiologically based risks for addiction, primarily alcohol use disorder
Effects of incidental stimulus exposure on cognition and behavior (i.e., priming effects).
The common theme around which these lines of work are integrated is the interplay between salience (i.e., motivational significance) and cognitive control (see Inzlicht, Bartholow, & Hirsch, 2015 ).
Salience, Cognitive Control, and Social Behavior
The interaction of salience and cognitive control is an enduring area of interest in the SCANlab, going back to Dr. Bartholow’s undergraduate days. In his undergraduate senior honors thesis, Dr. Bartholow found that participants asked to read résumés later recalled more gender-inconsistent information about job candidates. This general theme carried through to Dr. Bartholow’s dissertation research, in which he used event-related brain potentials (ERPs) to examine the neurocognitive consequences of expectancy violations. In that study, expectancy-violating behaviors elicited a larger P3-like positivity in the ERP and were recalled better compared to expectancy-consistent behaviors ( Bartholow et al., 2001 , 2003 ). Back then, we interpreted this effect as evidence for context updating (the dominant P3 theory at the time). As theoretical understanding of the P3 has evolved, we now believe this finding reflects the fact that unexpected information is salient, prompting engagement of controlled processing (see Nieuwenhuis et al., 2005 ).
Our research has been heavily influenced by cognitive neuroscience models of the structure of information processing, especially the continuous flow model ( Coles et al., 1985 ; Eriksen & Schultz, 1979) and various conflict monitoring theories (e.g., Botvinick et al., 2001 ; Shenhav et al., 2016 ). In essence, these models posit (a) that information about a stimulus accumulates gradually as processing unfolds, and (b) as a consequence, various stimulus properties or contextual features can energize multiple, often competing responses simultaneously, leading to a need to engage cognitive control to maintain adequate performance. This set of basic principles has influenced much of our research across numerous domains of interest (see Bartholow, 2010 ).
Applied to social cognition, these models imply that responses often classified as “automatic” (e.g., measures of implicit attitudes) might be influenced by control. We first tested this idea in the context of a racial categorization task in which faces were flanked by stereotype-relevant words ( Bartholow & Dickter, 2008 ). In two experiments, we found that race categorizations were faster when faces appeared with stereotype-congruent versus –incongruent words, especially when stereotype-congruent trials were more probable. Further, the ERP data showed that that this effect was not due to differences in the evaluative categorization of the faces (P3 latency), but instead reflected increased response conflict (N2 amplitude) due to partial activation of competing responses (lateralized readiness potential; LRP) on stereotype-incongruent trials. A more recent, multisite investigation (funded by the National Science Foundation ) extended this work by testing the role of executive cognitive function (EF) in the expression of implicit bias. Participants (N = 485) completed a battery of EF measures and, a week later, a battery of implicit bias measures. As predicted, we found that expression of implicit race bias was heavily influenced by individual differences in EF ability ( Ito et al., 2015 ). Specifically, the extent to which bias expression reflected automatic processes was reduced as a function of increases in general EF ability.
Another study demonstrating the role of conflict and control in “implicit” social cognition was designed to identify the locus of the affective congruency effect ( Bartholow et al., 2009 ), wherein people are faster to categorize the valence of a target if it is preceded by a valence-congruent (vs. incongruent) prime. This finding traditionally has been explained in terms of automatic spreading of activation in working memory (e.g., Fazio et al., 1986 ). By measuring ERPs while participants completed a standard evaluative priming task, we showed (a) that incongruent targets elicit response conflict; (b) that the degree of this conflict varies along with the probability of congruent targets, such that (c) when incongruent targets are highly probable, congruent targets elicit more conflict (also see Bartholow et al., 2005 ); and (d) that this conflict is localized to response generation processes, not stimulus evaluation.
Salience, Cognitive Control, and Alcohol
Drinking alcohol is inherently a social behavior. Alcohol commonly is consumed in social settings, possibly because it facilitates social bonding and group cohesion ( Sayette et al., 2012 ). Many of the most devastating negative consequences of alcohol use and chronic heavy drinking also occur in the social domain. Theorists have long posited that alcohol’s deleterious effects on social behavior stem from impaired cognitive control. Several of our experiments have shown evidence consistent with this idea, in that alcohol increases expression of race bias due to its impairment of control-related processes ( Bartholow et al., 2006 , 2012 ).
But exactly how does this occur? One answer, we believe, is that alcohol reduces the salience of events, such as a control failure (i.e., an error), that normally spur efforts at increased control. Interestingly, we found ( Bartholow et al., 2012 ) that alcohol does not reduce awareness of errors, as others had suggested ( Ridderinkhof et al., 2002 ), but rather reduces the salience or motivational significance of errors. This, in turn, hinders typical efforts at post-error control adjustment. Later work further indicated that alcohol’s control-impairing effects are limited to situations in which control has already failed, and that recovery of control following errors takes much longer when people are drunk ( Bailey et al., 2014 ). Thus, the adverse consequences people often experience when intoxicated might stem from alcohol’s dampening of the typical “affect alarm,” seated in the brain’s salience network (anterior insula and dorsal anterior cingulate cortex), which alerts us when control is failing and needs to be bolstered ( Inzlicht et al., 2015 ).
Incidental Stimulus Exposure Effects
A fundamental tenet of social psychology is that situational factors strongly affect behavior. Despite recent controversies related to some specific effects, we remain interested in the power of priming, or incidental stimulus exposure, to demonstrate this basic premise. We have studied priming effects in numerous domains, including studies showing that exposure to alcohol-related images or words can elicit behaviors often associated with alcohol consumption, such as aggression and general disinhibition.
Based on the idea that exposure to stimuli increases accessibility of relevant mental content ( Higgins, 2011 ), we reasoned that seeing alcohol-related stimuli might not only bring to mind thoughts linked in memory with alcohol, but also might instigate behaviors that often result from alcohol consumption. As an initial test of this idea, in the guise of a study on advertising effectiveness we randomly assigned participants to view magazine ads for alcoholic beverages or for other grocery items and asked them to rate the ads on various dimensions. Next, we asked participants if they would help us pilot test material for a future study on impression formation by reading a paragraph describing a person and rating him on various traits, including hostility. We reasoned that the common association between alcohol and aggression might lead to a sort of hostile perception bias when evaluating this individual. As predicted, participants who had seen ads for alcohol rated the individual as more hostile than did participants who had seen ads for other products, and this effect was larger among people who had endorsed (weeks previously) the notion that alcohol increases aggression ( Bartholow & Heinz, 2006 ). Subsequently, this finding has been extended to participants’ own aggression in verbal ( Friedman et al., 2007 ) and physical domains ( Pedersen et al., 2014 ), and has been replicated in other labs (e.g., Bègue et al., 2009 ; Subra et al., 2010 ).
Of course, aggression is not the only behavior commonly assumed to increase with alcohol. Hence, we have tested whether this basic phenomenon extends into other behavioral domains, and found similar effects with social disinhibition ( Freeman et al., 2010 ), tension-reduction (Friedman et al., 2007), race bias ( Stepanova et al., 2012 , 2018 a, 2018 b), and risky decision-making (Carter et al., in prep.). Additionally, it could be that participants are savvy enough to recognize the hypotheses in studies of this kind when alcohol-related stimuli are presented overtly (i.e., experimental demand). Thus, we have also tested the generality of the effect by varying alcohol cue exposure procedures, including the use of so-called “sub-optimal” exposures (i.e., when prime stimuli are presented too quickly to be consciously recognized). Here again, similar effects have emerged (e.g., Friedman et al., 2007; Loersch & Bartholow, 2011 ; Pedersen et al., 2014).
Taken together, these findings highlight the power of situational cues to affect behavior in theoretically meaningful ways. On a practical level, they point to the conclusion that alcohol can affect social behavior even when it is not consumed, suggesting, ironically, that even nondrinkers can experience its effects.
Aberrant Salience and Control as Risk Factors for Addiction
Salience is central to a prominent theory of addiction known as incentive sensitization theory (IST; e.g., Robinson & Berridge, 1993 ). Briefly, IST posits that, through use of addictive drugs, including alcohol, people learn to pair the rewarding feelings they experience (relaxation, stimulation) with various cues present during drug use. Eventually, repeated pairing of drug-related cues with reward leads those cues to take on the rewarding properties of the drug itself. That is, the cues become infused with incentive salience, triggering craving, approach and consummatory behavior.
Research has shown critical individual differences in vulnerability to attributing incentive salience to drug cues, and that vulnerable individuals are at much higher risk for addiction. Moreover, combining incentive sensitization with poor cognitive control (e.g., during a drinking episode) makes for a “potentially disastrous combination” ( Robinson & Berridge, 2003 , p. 44). To date, IST has been tested primarily in preclinical animal models. Part of our work aims to translate IST to a human model.
In a number of studies over the past decade, we have discovered that a low sensitivity to the effects of alcohol (i.e., needing more drinks to feel alcohol’s effects), known to be a potent risk factor for alcoholism, is associated with heightened incentive salience for alcohol cues. Compared with their higher-sensitivity (HS) peers, among low-sensitivity (LS) drinkers alcohol-related cues (a) elicit much larger neurophysiological responses ( Bartholow et al., 2007 , 2010 ; Fleming & Bartholow, in prep.); (b) capture selective attention ( Shin et al., 2010 ); (c) trigger approach-motivated behavior ( Fleming & Bartholow, 2014 ); (d) produce response conflict when relevant behaviors must be inhibited or overridden by alternative responses ( Bailey & Bartholow, 2016 ; Fleming & Bartholow, 2014), and (e) elicit greater feelings of craving (Fleming & Bartholow, in prep.; Piasecki et al., 2017 ; Trela et al., in press). These findings suggest that LS could be a human phenotype related to sign-tracking , a conditioned response reflecting susceptibility to incentive sensitization and addiction ( Robinson et al., 2014 ).
Recently, our lab has conducted two major projects designed to examine how the incentive salience of alcohol-related cues is associated with underage drinking. One such project, funded by the National Institute on Alcohol Abuse and Alcoholism (NIAAA; R01-AA020970 ), examined the extent to which pairing beer brands with major U.S. universities enhances the incentive salience of those brands for underage students. Major brewers routinely associate their brands with U.S. universities through direct marketing and by advertising during university-related programming (e.g., college sports). We tested whether affiliating a beer brand with students’ university increases the incentive salience of the brand, and whether individual differences in the magnitude of this effect predict changes in underage students’ alcohol use. We found (a) that P3 amplitude elicited by a beer brand increased when that brand was affiliated with students’ university, either in a contrived laboratory task or by ads presented during university-related sports broadcasts; (b) that stronger personal identification with the university increased this effect; and (c) that variability in this effect predicted changes in alcohol use over one month, controlling for baseline levels of use ( Bartholow et al., 2018 ).
A current project, also funded by the NIAAA ( R01-AA025451 ), aims to connect multiple laboratory-based measures of the incentive salience of alcohol-related cues to underage drinkers’ reports of craving, alcohol use, and alcohol-related consequences as they occur in their natural environments. This project will help us to better understand the extent to which changes in drinking lead to changes in alcohol sensitivity and to corresponding changes in the incentive salience of alcohol-related cues.
- Research article
- Open access
- Published: 20 May 2024
Clinical differences between periprosthetic and native distal femur fractures: a comparative observational study
- Shana Kong 1 ,
- Shannon Tse 1 ,
- Aziz Saade 1 ,
- Barry Bautista 1 ,
- Max Haffner 1 &
- Augustine M. Saiz Jr. 1
Journal of Orthopaedic Surgery and Research volume 19 , Article number: 303 ( 2024 ) Cite this article
Metrics details
Introduction
The incidence of periprosthetic distal femur fractures (PDFF) is increasing as the number of total knee replacements becomes more common. This study compared the demographics, fracture characteristics, treatment, and outcomes of periprosthetic versus native distal femur fractures (NDFF).
Materials and methods
This was a retrospective cohort study of patients ≥ 18 who underwent surgical fixation of NDFF or PDFF from 2012 to 2020 at a level-1 trauma center. The main variables collected included demographics, AO/OTA fracture classification, fixation construct, concomitant fractures, polytrauma rates, bone density, and reduction quality. Primary outcomes were unexpected return to the operating room (UROR), hospital length of stay, and quality of reduction. T-tests, Fisher’s exact tests, and multivariate analyses were used for statistical analysis.
209 patients were identified, including 70 PDFF and 139 NDFF. PDFF patients were elderly females (81%) with isolated (80%) and comminuted (85%) 33 A.3 (71%) fractures. NDFF patients included 53% females, were commonly middle-aged, and displayed comminuted (92%) 33 C.2 fractures. 48% of NDFF patients had concomitant fractures. Intramedullary nailing was the primary fixation for both groups, followed by nail-plate combination (37%) for PDFF and lateral locking plates (21%) for NDFF. NDFF patients experienced significantly longer hospital stays, higher UROR rates, and worse quality of reduction ( p < 0.05). PDFF patients had a significantly greater prevalence of low bone density ( p < 0.05).
PDFF occur as isolated injuries with significant metaphyseal comminution in elderly females with low bone quality. NDFF commonly occurs in younger patients with less metaphyseal comminution and concomitant fractures. Intramedullary nailing was the most common treatment for both groups, although preference for nail-plate combination fixation is increasing. NDFF type 33 C fractures are at greater risk of UROR.
In 2012, total knee arthroplasty (TKA) was the single most common surgical procedure performed in the United States, with 94% of those procedures occurring in patients 65–84 years old [ 1 , 2 ]. As the population ages and the prevalence of TKA rises, the frequency of periprosthetic distal femur fractures (PDFF) has simultaneously increased. Multiple studies report that periprosthetic distal femur fractures are not uncommon following TKA [ 3 , 4 , 5 ]. Court-Brown et al. reported an increase in PDFF prevalence from 15.4 to 27.8% of all distal femur fractures from 2007 to 2011 [ 6 ]. Treatment of PDFF presents a challenge for orthopedic surgeons, who must consider not only the complex and variable fracture morphology associated with the prosthesis but also the specific populations at risk.
Previous studies have focused on analyzing PDFF and native distal femur fractures (NDFF) separately. Roy et al. analyzed NDFF exclusively at a single level-1 trauma center and characterized the affected population as middle-aged, female (66%), and more often overweight than osteoporotic [ 7 ]. Additionally, they identified similar rates of high-and low-energy trauma in their NDFF cohort and found that high-energy injuries were associated with more severe fracture types (AO/OTA 33B/C), open fractures, and additional orthopedic injuries, while low-energy injuries were associated with closed fractures and less severe fracture types (AO/OTA 33 A) [ 7 ]. Elsoe et al. first reported on the demographics of PDFF, noting a population distribution of elderly females (mean age = 77) with low-energy injuries [ 8 ]. Regarding treatment, lateral plating and retrograde intramedullary nailing (rIMN) have been reported as the most common and successful fixation methods for both PDFF and NDFF, although intramedullary nail-plate combination (NPC) fixation is a more recent technique developed to allow quicker weight bearing and achieve better purchase in osteoporotic bone [ 7 , 9 , 10 , 11 , 12 ]. Studies have reported similar 30-day and 90-day outcomes [ 13 , 14 ]. A previous case series reported that osteoporosis, comminution, intra-articular involvement, and soft tissue injury in open fractures were associated with worse long-term (> 5 years) outcomes such as malunion, nonunion, and infection in NDFF [ 15 ]. Reduction quality has yet to be studied in either group.
In the existing body of literature, there is a notable lack of comprehensive comparisons between PDFF and NDFF within single institutions. Studies have focused exclusively on one fracture type without directly comparing it with the other. As a result, there is limited understanding of the relative differences between PDFF and NDFF in terms of demographics, fracture characteristics, treatment modalities, and outcomes, as patients from both groups can only be compared from different studies, which potentially raises concerns such as selection bias, confounding, heterogeneity, and timeframe variations with historical comparisons.
While there is some consistency in the literature regarding these fracture types, there remains a need to systematically examine and compare them within the same population to further denote the remaining discrepancies which may arise from limited generalizability. Therefore, the primary objective of this study was to conduct a detailed comparison of PDFF and NDFF using data from a single institution. This paper contributes to our understanding of the differences in patient populations, specific injury patterns, and treatment strategies between periprosthetic and native distal femur fractures. Such insights are valuable for patient counseling. Moreover, attempting to adapt fixation strategies from one to the other may prove ineffective, thus prompting avenues for further exploration.
A secondary aim was to explore aspects such as the quality of reduction and long-term outcomes, which have not been extensively studied in prior literature. NDFF often have more complex fracture morphology and are not only more difficult to reduce but are further complicated by the need to restore length, planar alignment, and joint line congruity. In contrast, PDFF tend to be simpler fractures, but it can be challenging to achieve anchorage and maintain adequate fixation in highly comminuted, osteoporotic bone [ 16 ]. Studying reduction quality and long-term outcomes in these groups would provide valuable insight on whether current treatment strategies are achieving optimal fixation for both groups, and could guide future, more personalized treatment strategies to improve patient outcomes.
We hypothesize that PDFF are more likely to be isolated, simple, low-energy, injuries experienced by elderly patients while NDFF will be experienced by a younger population and result in more complicated fracture patterns due to higher levels of trauma.
Furthermore, we hypothesize that there will be no difference in postoperative outcomes between PDFF and NDFF groups.
Cohort selection
This retrospective study was approved by the Institutional Review Board. All patients who were at least 18 years of age at the time of admission with distal femur fractures between January 2012 and December 2020 at a single level-1 trauma center were identified. These patients were later classified as either NDFF or PDFF. Patients with bilateral distal femur fractures were excluded.
Data collection
Electronic medical records were used to obtain clinical and demographic data for each patient. American Society of Anesthesiologists (ASA) score and bone density status were obtained from clinical records. Presence of bone loss, classified as either osteopenia or osteoporosis, was determined by either previous diagnosis documented in the patient chart with a prior DEXA scan or by comments noted by radiologists from existing radiographs following a fragility fracture. Fracture characteristics, including AO/OTA fracture classification, were obtained from preoperative radiographs (Figs. 1 and 2 ) and computed tomography (CT) scans. Polytrauma was noted if present and defined as having two or more injuries affecting two or more bodily areas. Type of surgical fixation was obtained from operative notes and postoperative radiographs (Figs. 1 and 2 ). Patients with NPC fixation were categorized separately and did not contribute to nail or plate counts. Primary outcomes were unexpected return to the operating room (UROR), hospital length of stay, and quality of reduction. Postoperative outcome data was obtained using follow-up notes and postoperative radiographs.

Preoperative (left) and post-IMN (right) NDFF radiographs

Preoperative (left) and post-NPC (right) PDFF radiographs
Quality of reduction was assessed by calculating the difference in alignment from the population average anatomic lateral distal femoral angle (aLDFA) on postoperative anteroposterior (AP) radiographs. These measurements were made by a single trained grader. To measure the aLDFA (Fig. 3 ), a line was first drawn parallel to both femoral condyles of the affected femur, representing the knee joint line. Next, a line was drawn from the center of the femoral head to the intercondylar notch of the affected femur, representing the mechanical axis of the femur. The lateral angle formed between the mechanical axis of the femur and the knee joint line was recorded in degrees as the aLDFA. The aLDFA for the contralateral, unaffected femur was also calculated for use as a reference for each patient if contralateral films had been acquired. The mean difference from the published population average aLDFA of 81 degrees was calculated in the affected and unaffected femurs for both PDFF and NDFF groups [ 16 , 17 , 18 , 19 ]. A smaller deviation from the population average aLDFA was accepted as a more desirable outcome.

Measurement of aLDFA on AP radiographs
Statistical analyses
Differences between PDFF and NDFF patients were compared using Fisher’s exact tests, unpaired t-tests, or multivariate analyses, as appropriate for each variable using Microsoft Excel. Multivariate analysis was completed in Excel using a linear regression with all variables included. Results were described using incidence rates, means, and one standard deviation. A p-value < 0.05 indicated statistical significance.
In total, 209 patients were included in this study. Table 1 summarizes the preoperative characteristics of both cohorts. The mean age of NDFF patients was 23 years younger than the PDFF patients ( p < 0.001). There were significantly fewer females in the NDFF cohort (53% compared to 81%, p < 0.001). The PDFF cohort had significantly higher rates of bone loss (55.7% compared to 19.4%, p < 0.001). There was no significant difference between the ASA scores of the two cohorts ( p = 0.061).
Table 2 summarizes the fracture characteristics of the two cohorts. 33 A.2 and 33 A.3 classifications represented the entirety of PDFF. In comparison, NDFF AO/OTA classifications were represented by 33 C.2 (28%), 33 C.3 (22%), and 33B.1 (12%), which were significantly more prevalent than in the PDFF cohort ( p < 0.001 for 33 C.2 and 33 C.3, and p < 0.05 for 33B.1).
Table 2 also shows significant differences in the rate of isolated injuries and polytraumas between both cohorts. PDFF were more often isolated injuries in patients (80% versus 51.8%, p < 0.001). NDFF patients were more likely to be polytraumatized (41% compared to 18.6%, p < 0.001). Additionally, NDFF patients had higher rates of open fractures (30.7% compared to 11.2%, p = 0.002). Out of 43 open NDFF fractures, 77% were Gustilo-Anderson type III open fractures (31 type 3 A, 2 type 3 C), 14% type II fractures, and 9% type I fractures (Table 2 ).
Of these open fractures, 41 underwent definitive fixation at first operation while 2 initially underwent external fixation due to the presence of an unstable knee (multiligamentous injury, fracture-dislocation). Out of 8 open PDFF fractures, 50% were Gustilo-Anderson type II, 25% type III, and 25% type I (Table 2 ). Only one PDFF patient was initially temporized with an external fixator before definitive fixation. There was no significant difference between the comminution rates of fractures in both cohorts ( p = 0.274).
Table 3 summarizes the surgical fixation constructs used for both cohorts. Retrograde intermedullary nail was the most common fixation utilized in both groups, and there was no significant difference in the prevalence of rIMN between the two groups (NDFF = 36.7%, PDFF = 44.3%, p = 0.297). NDFF patients had significantly higher rates of medial plate fixation (5.8% compared to 0%, p < 0.05) and PDFF patients had significantly higher rates of NPC fixation (37.1% compared to 17.2%, p < 0.05). Further analysis of NPC fixation revealed usage beginning in 2015 for both groups, with prevalence of usage increasing from 3.3% and 0.7–13.3% and 4.3% in 2019 (PDFF) and 2020 (NDFF) respectively. Of 13 PDFF that received plate fixation, only 2 had fracture patterns amenable for nail fixation but preexisting implants (long-stemmed proximal component, Schneider rods for osteogenesis imperfecta) precluded intramedullary fixation. The 11 PDFF patients that received plate fixation had stable femoral components and fracture morphology that could not be effectively reduced with intramedullary fixation.
Postoperative outcomes are summarized in Table 4 . Patients in the NDFF cohort had an approximately five-day longer length of stay compared to those in the PDFF cohort ( p < 0.05). This was most likely because NDFF patients had more polytrauma (41% vs. 18.6%, p < 0.001) and open injuries (30.7% vs. 11.2%, p = 0.002) There was no significant difference in length of follow-up between the two cohorts ( p = 0.564). Postoperatively, PDFF were significantly more likely to be weight bearing as tolerated (WBAT) compared to partial weight bearing (PWB) or non-weight bearing (NWB). NDFF postoperative weight bearing status consisted of 60% NWB, 21% WBAT, and 19% PWB. There was some correlation between postoperative weight bearing status and fixation. All NDFF patients who were WBAT underwent IMN, NPC, or lag screw fixation. Of patients who were NWB, 50% received plate fixation. There was no significant difference in WBAT assignment for NDFF who received NPC vs. nail or plate fixation alone ( p = 0.88).
For NDFF patients who were NWB or PWB, there was no correlation with fixation. However, there was a correlation between weight bearing status and polytrauma. Rates of polytrauma were 99% and 52% in patients who were NWB and PWB, respectively. Additionally, a majority of patients (60%) who received IMN fixation and were PWB had concomitant extremity fractures, preventing them from having increased weight bearing.
PDFF postoperative weight bearing status consisted of 60% WBAT, 30% PWB, and 10% NWB. Again, there was some correlation between postoperative weight bearing status and fixation. 100% of patients who were WBAT underwent IMN or NPC fixation, while 50% of patients who were TDWB underwent plate fixation. PDFF that received NPC fixation were significantly more likely to be assigned WBAT compared to those that underwent nail or plate fixation alone ( p < 0.05). For patients who were PWB or NWB, there was no correlation between postoperative weight bearing status and fixation.
Compared to their PDFF counterparts, NDFF patients had higher rates of any unexpected return to the operating room (UROR) occurrences (13.6% compared to 8.5%, p < 0.05). Among the 19 NDFF requiring reoperation, 10 (52%) were AO/OTA type 33 C fractures. Irrigation and debridement (I&D) of the femur fracture of interest due to infection was the leading cause of UROR for NDFF patients (5% compared to 0%). NDFF UROR patients that initially experienced open fractures had a significantly greater risk of returning for I&D compared to closed NDFF fractures, likely due to an increased risk for infection ( p < 0.05, Table 5 ). The most common reason for revision operation within the NDFF cohort was due to the intra-articular prominence of an intramedullary nail, and the other revision within the PDFF cohort was due to implant failure with valgus angulation. PDFF patients had significantly improved quality of reduction with respect to the average population aLDFA of 81 degrees. The mean aLDFA in PDFF patients was approximately 6 degrees less than that of NDFF patients ( p < 0.001). When using the uninjured contralateral aLDFA, PDFF were approximately 1.2 degrees less in deviation. However, significance could not be determined given the limited availability of contralateral imaging.
Of 26 PDFF treated with NPC fixation, only 1 (4%) experienced long-term post-operative complications of malunion. Of 44 PDFF treated with either nail or plate fixation, 2 (4.5%) experienced postoperative complications of nonunion. There was no significant difference in malunion/nonunion rates between these two groups ( p = 0.88).
All 24 NDFF treated with NPC fixation achieved fracture union. Of 115 NDFF treated with either nail or plate fixation, 5 experienced malunion/nonunion. There was no significant difference in malunion/nonunion rates between NDFF treated with NPC fixation compared to either plate or nail fixation ( p = 0.59).
This study is the first to directly compare native and periprosthetic distal femur fractures. PDFF were found to be commonly isolated injuries with complete metaphyseal comminution, affecting elderly women and those with low bone quality. NDFF, on the other hand, tended to occur in younger patients with less metaphyseal comminution and additional fractures. NDFF had increased revision reoperation rates compared to PDFF, specifically for I&D of the femur fracture of interest. In addition to having generally more open fractures in the NDFF group, patients with open fractures within the NDFF group were more likely to result in infection requiring I&D than those with closed fractures. Multivariate regression analysis revealed that NDFF were an independent risk factor for reoperation, specifically I&D of the fracture of interest, compared to PDFF.
The present study reports a PDFF gender distribution similar to Elsoe et al., who documented a sample of mostly females with a mean age of 77 years old [ 8 ]. Generally, our PDFF sample was characterized by a high prevalence of low bone density. Additionally, the PDFF cohort had a higher rate of low bone density compared to the NDFF cohort, which can be explained by the higher average age and the female majority in the PDFF group [ 20 ]. Low bone density has been highlighted as a risk factor for femur fractures in past studies, and low-energy distal femur fractures are now considered fragility fractures [ 6 , 21 ]. Although trauma mechanisms were not formally investigated in our study, we observed that PDFF were mostly isolated injuries, which is more suggestive of a low-energy trauma mechanism as proposed by prior studies [ 7 , 22 ].
The most common fracture pattern for PDFF was extraarticular with complete metaphyseal comminution (AO/OTA 33 A.3). The increased metaphyseal comminution is likely related to both the presence of low bone quality and the TKA implant affecting the stress concentration locations of the fracture. Low bone quality leads to an overall decreased tolerance for withstanding forces. Additionally, with the presence of a TKA, the fracture cannot propagate into the joint, and more energy may be imparted to the metaphysis.
While previous studies have shown that rIMN and lateral locked plating are the most common methods for treating PDFF, our study revealed that rIMN and NPC fixation are the most common methods utilized at our institution [ 10 , 23 , 24 ]. Further analysis of NPC fixation rates revealed an increase in prevalence from 3.3% in 2015 to 13.3% of all fixation constructs used for PDFF in 2019. There was no significant difference in malunion/nonunion rates for those treated with NPC fixation compared to those treated with rIMN or plate fixation alone for either NDFF or PDFF. Regarding postoperative weightbearing status, there was no significant difference in WBAT assignment for NDFF NPC fixation compared to nail or plate fixation ( p = 0.88). This was likely confounded by the high prevalence of polytrauma and concomitant fractures in this group, which would have limited weightbearing. However, PDFF treated with NPC fixation were significantly more likely to be WBAT compared to those treated with nail or plate fixation alone ( p < 0.05). NPC fixation is a recently being used as an ideal treatment for osteoporotic distal femur fractures (both PDFF and NDFF) due to the balanced energy distribution between bone and implant [ 25 ]. Currently, only small cohort studies exist which have found no significant difference in nonunion rates between NPC compared to nail or plate fixation, although a multicenter propensity analysis suggested there may be significantly lower nonunion rates in DFF treated with NPC fixation [ 25 , 26 , 27 ]. In addition to potentially reducing the risk of nonunion, many surgeons see a biomechanical advantage of combination fixation to facilitate early weightbearing in elderly patients [ 25 ]. It is of the authors’ opinion that the results reflect an increasing preference for this treatment by orthopedic surgeons at our institution to stabilize fractures in elderly patients with low bone density to facilitate earlier mobilization/weight bearing.
We have identified a large NDFF population of middle-aged patients (average age = 57 years old) with a balanced sex distribution. The most common fracture pattern consisted of metaphyseal comminution with intra-articular extension (AO/OTA 33 C.2), suggesting a predominantly high-energy trauma mechanism. This contrasts with the findings of Roy et al., who reported a small sample of NDFF at a level-1 trauma center ( n = 87) consisting mostly of middle-aged female patients with comparable rates of high-energy (47%) and low-energy injuries (53%) [ 28 ]. These differences may be reflective of differences in the demographics of the catchment area that our institution serves.
In contrast to prior literature, which reports coronal plane (AO/OTA 33B.3) fractures representing 38% of all partial articular (AO/OTA 33B) native fractures, our study reports an overall rate of 14% for 33B fractures with a majority being fractures of the lateral condyle (AO/OTA 33B.1) [ 29 ]. The mechanism of coronal plane fractures consists of vertical shear forces experienced during high-energy trauma, which is consistent with our findings in the NDFF population. The difference in our reported prevalence of 33B.3 fractures is less likely to be explained by low detection as CT scans were obtained for all patients. These demographic and injury severity differences may be reflective of population differences in sampling; however, we report an NDFF cohort that is much larger than the previously mentioned study, with greater potential for generalizability.
Regarding the treatment of NDFF, rIMN was also the most common fixation method used, followed by lateral plating, which contrasts with previous studies which report plating as the most common fixation for NDFF [ 7 , 11 , 12 ]. Additionally, NPC was the third most common construct employed, which may reflect its increasing popularity as a treatment alternative for distal femur fractures as well as institutional preference for nailing.
Quality of reduction was improved in the PDFF cohort compared to the NDFF cohort, based on normative values of alignment. This may be due to the simplicity of the fractures as PDFF were all type A fractures whereas NDFF commonly had intra-articular components. Additionally, the TKA implants force a certain nail start point given the box component with less variation so perhaps the nail is more on axis. However, nailing of these fractures has been previously associated with malalignment [ 30 , 31 ]. Finally, the increase in NPC versus lateral plating alone may account for some of the differences as the tendency for malreduction with a single lateral locked plate is well documented [ 32 ]. We did not observe any difference in nonunion, similar to prior studies but with an overall lower rate [ 30 ].
Contrary to our hypothesis, there were notable differences in outcomes between NDFF and PDFF. NDFF had significantly longer length of stays and were more likely to return to the operating room for additional treatment of the femur fracture compared to PDFF. The most common fracture pattern seen in NDFF undergoing reoperation was complete articular (AO/OTA 33 C), and the most common etiology for UROR was for irrigation and debridement of an initially open fracture due to infection risk, which is reflective of the more severe soft tissue injury and propensity for open fractures. Upfill-Brown et al. previously conducted a large retrospective review which found no significant differences in 30-day reoperation rates between PDFF and NDFF [ 13 ]. However, their study did not account for mechanism or fracture complexity. The differences in length of stay and UROR rates between the PDFF and NDFF groups noted in our study can be explained by the high prevalence of polytrauma, additional fractures, and increased fracture complexity (AO/OTA 33 C) in the NDFF group. Additionally, Kaufman et al. studied outcomes in a matched cohort of PDFF and NDFF and found that when controlling for age, sex, and injury severity, there was no significant difference in length of stay or < 90-day readmission rates between the two injuries [ 14 ]. The results of Kaufman et al. and our study support the notion that the risk for readmission is more closely tied to population-specific risk factors such as demographics, mechanism, and additional injuries than to the presence of periprosthetic fractures.
There are several notable strengths to this study. This investigation encompasses recent patient data from a large population spanning 8 years followed longitudinally. Our study takes into consideration the quality of reduction when assessing outcomes for PDFF and NDFF. Limitations to the study include retrospective-single site sampling and an unmatched patient cohort. Reduction quality measurements were made by a single grader, potentially introducing information bias. Our results reflect the treatment of distal femur fractures at a level-1 trauma center, and it is unclear whether similar results would be observed at a community hospital or arthroplasty surgical center. Finally, the addition of patient-reported outcomes would be beneficial but were not collected during the time frame investigated.
In conclusion, there are differences in the patient demographics, fracture patterns, and fixation construct strategies of PDFF and NDFF patient populations. PDFF frequently occur as isolated, extra-articular, and comminuted injuries. Elderly women and those with poor bone quality are at high risk for PDFF. NDFF often occur in middle-aged individuals of both genders, often involving intra-articular extension and are frequently accompanied by additional orthopedic injuries. Patients with NDFF are at a significantly greater risk of reoperation, particularly due to soft tissue complications from open fractures. Finally, although rIMN was the common fixation strategy for both fracture categories, rates of NPC fixation for PDFF are increasing at our institution, likely to facilitate earlier weight bearing in elderly, nonpolytraumatized patients with qualifying fracture morphology. These differences can guide future research to enhance treatment algorithms and implant designs specific to each population, ultimately improving patient outcomes.
Data availability
No datasets were generated or analysed during the current study.
Fingar KR, Truven Health Analytics). (Stocks C (AHRQ), Weiss AJ (Truven Health Analytics), Steiner CA (AHRQ). Most Frequent Operating Room Procedures Performed in U.S. Hospitals, 2003–2012. HCUP Statistical Brief #186. December 2014. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb186-Operating-Room-Procedures-United-States-2012.pdf .
Benkovich V, Klassov Y, Mazilis B, Bloom S. Periprosthetic fractures of the knee: a comprehensive review. Eur J Orthop Surg Traumatol. 2020;30(3):387–399. doi: 10.1007/s00590-019-02582-5. Epub 2019 Nov 19. PMID: 31745642; PMCID: PMC7138771.
Welch T, Iorio R, Marcantonio AJ, Kain MS, Tilzey JF, Specht LM, Healy WL. Incidence of Distal Femoral Periprosthetic Fractures after Total Knee Arthroplasty. Bull Hosp Jt Dis (2013). 2016;74(4):287–292. PMID: 27815952.
Rorabeck CH, Taylor JW. Periprosthetic fractures of the femur complicating total knee arthroplasty. Orthop Clin North Am. 1999;30(2):265 – 77. https://doi.org/10.1016/s0030-5898(05)70081-x . PMID: 10196428.
Berry DJ. Epidemiology: hip and knee. Orthop Clin North Am. 1999;30(2):183 – 90. https://doi.org/10.1016/s0030-5898(05)70073-0 . PMID: 10196420.
Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury. 2006;37(8):691–7. https://doi.org/10.1016/j.injury.2006.04.130 . Epub 2006 Jun 30. PMID: 16814787.
Article PubMed Google Scholar
Roy D, Ramski D, Malige A, Beck M, Jeffers K, Brogle P. Injury patterns and outcomes associated with fractures of the native distal femur in adults. Eur J Trauma Emerg Surg. 2021;47(4):1123–8. https://doi.org/10.1007/s00068-019-01287-y . Epub 2019 Dec 23. PMID: 31872341.
Elsoe R, Ceccotti AA, Larsen P. Population-based epidemiology and incidence of distal femur fractures. Int Orthop. 2018;42(1):191–6. https://doi.org/10.1007/s00264-017-3665-1 . Epub 2017 Nov 7. PMID: 29116356.
Ristevski B, Nauth A, Williams DS, Hall JA, Whelan DB, Bhandari M. Systematic review of the treatment of periprosthetic distal femur fractures. J Orthop Trauma. 2014;28(5):307 – 12. https://doi.org/10.1097/BOT.0000000000000002 . PMID: 24149447.
Ebraheim NA, Kelley LH, Liu X, Thomas IS, Steiner RB, Liu J. Periprosthetic distal femur fracture after total knee arthroplasty: a systematic review. Orthop Surg. 2015;7(4):297–305. https://doi.org/10.1111/os.12199 . PMID: 26790831; PMCID: PMC6583744.
Article PubMed PubMed Central Google Scholar
Tahami M, Vaziri AS, Tahmasebi MN, Vosoughi F, Khalilizad M, Shakiba S. Practical approach to the native distal femur fractures in the elderly: a rapid review over the recent trends. Injury. 2022;53(7):2389–94. https://doi.org/10.1016/j.injury.2022.05.014 . Epub 2022 May 19. PMID: 35644641.
Koso RE, Terhoeve C, Steen RG, Zura R. Healing, nonunion, and re-operation after internal fixation of diaphyseal and distal femoral fractures: a systematic review and meta-analysis. Int Orthop. 2018;42(11):2675–83. https://doi.org/10.1007/s00264-018-3864-4 . Epub 2018 Mar 8. PMID: 29516238.
Upfill-Brown A, Arshi A, Sekimura T, Lee C, Stavrakis A, Sassoon A. Short-term outcomes of periprosthetic compared to native distal femur fractures, a national database study. Arch Orthop Trauma Surg. 2021 Jun 29. https://doi.org/10.1007/s00402-021-04000-0 . Epub ahead of print. PMID: 34185154.
Kaufman MW, Rascoe AS, Hii JL, Thom ML, Levine AD, Wilber RG. Comparable outcomes between native and periprosthetic fractures of the distal femur. J Knee Surg. 2022 Jul;12. https://doi.org/10.1055/s-0042-1749604 . Epub ahead of print. PMID: 35820430.
Nasr AM, Mc Leod I, Sabboubeh A, Maffulli N. Conservative or surgical management of distal femoral fractures. A retrospective study with a minimum five year follow-up. Acta Orthop Belg. 2000;66(5):477–83. PMID: 11196372.
CAS PubMed Google Scholar
von Rüden C, Augat P. Failure of fracture fixation in osteoporotic bone. Injury. 2016;47 Suppl 2:S3-S10. https://doi.org/10.1016/S0020-1383(16)47002-6 . PMID: 27338224.
Mize RD, Bucholz RW, Grogan DP. Surgical treatment of displaced, comminuted fractures of the distal end of the femur. J Bone Jt Surg Am. 1982;64:871–9.
Article CAS Google Scholar
Schatzker J, Lambert DC. Supracondylar fractures of the femur. Clin Orthop Relat Res. 1979:77–83.
Keats TE, Teeslink R, Diamond AE, et al. Normal axial relationships of the major joints. Radiology. 1966;87:904–7.
Article CAS PubMed Google Scholar
Kanis JA. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report. WHO Study Group. Osteoporos Int. 1994;4(6):368 – 81. https://doi.org/10.1007/BF01622200 . PMID: 7696835.
Ng AC, Drake MT, Clarke BL, Sems SA, Atkinson EJ, Achenbach SJ. Trends in subtrochanteric, diaphyseal, and distal femur fractures, 1984–2007. Osteoporos Int. 2012;23(6):1721–6. https://doi.org/10.1007/s00198-011-1777-9 . Epub 2011 Sep 10. PMID: 21909727; PMCID: PMC3266989.
Pietu G, Lebaron M, Flecher X, Hulet C, Vandenbussche E, SOFCOT. Epidemiology of distal femur fractures in France in 2011-12. Orthop Traumatol Surg Res. 2014;100(5):545–8. https://doi.org/10.1016/j.otsr.2014.06.004 . Epub 2014 Aug 22. PMID: 25155091.
Lombardo DJ, Siljander MP, Sobh A, et al. Periprosthetic fractures about total knee arthroplasty. Musculoskelet Surg. 2020;104:135–43. https://doi.org/10.1007/s12306-019-00628-9 .
Nauth A, Ristevski B, Bégué T, Schemitsch EH. Periprosthetic distal femur fractures: current concepts. J Orthop Trauma. 2011;25 Suppl 2:S82-5. https://doi.org/10.1097/BOT.0b013e31821b8a09 . PMID: 21566481.
Liporace FA, Yoon RS. Nail Plate Combination Technique for Native and Periprosthetic Distal Femur Fractures. J Orthop Trauma. 2019;33(2):e64-e68. https://doi.org/10.1097/BOT.0000000000001332 . PMID: 30277982.
Passias BJ, Emmer TC, Sullivan BD, Gupta A, Myers D, Skura BW, Taylor BC. Treatment of Distal Femur Fractures with a Combined Nail-Plate Construct: Techniques and Outcomes. J Long Term Eff Med Implants. 2021;31(3):15–26. https://doi.org/10.1615/JLongTermEffMedImplants.2021038016 . PMID: 34369718.
Shi BY, Brodke DJ, O’Hara N, Devana S, Hernandez A, Burke C, Gupta J, McKibben N, O’Toole R, Morellato J, Gillon H, Walters M, Barber C, Perdue P, Dekeyser G, Steffenson L, Marchand L, Shymon S, Fairres MJ, Black L, Working Z, Roddy E, El Naga A, Hogue M, Gulbrandsen T, Atassi O, Mitchell T, Lee C. Nail Plate Combination Fixation Versus Lateral Locked Plating for Distal Femur Fractures: A Multicenter Experience. J Orthop Trauma. 2023;37(11):562–567. https://doi.org/10.1097/BOT.0000000000002661 . PMID: 37828687.
Bretin P, O’Loughlin PF, Suero EM, et al. Influence of femoral malrotation on knee joint alignment and intra-articular contract pressures. Arch Orthop Trauma Surg. 2011;131:1115–20.
Nork SE, Segina DN, Aflatoon K, Barei DP, Henley MB, Holt S. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. The Journal of Bone & Joint Surgery 87(3):p 564–569, March 2005. | https://doi.org/10.2106/JBJS.D.01751 .
Gausden EB, Lim PK, Rabonivich A, Shaath MK, Mitchell PM, Hartline B. Outcomes of periprosthetic distal femur fractures following total knee arthroplasty: Intramedullary nailing versus plating. Injury. 2021;52(7):1875–9. https://doi.org/10.1016/j.injury.2021.05.007 . Epub 2021 May 12. PMID: 34030866.
Campbell ST, Lim PK, Kantor AH, Gausden EB, Goodnough LH, Park AY. Complication rates after lateral plate fixation of Periprosthetic Distal Femur fractures: a Multicenter Study. Injury. 2020;51(8):1858–62. https://doi.org/10.1016/j.injury.2020.05.009 . Epub 2020 May 22. PMID: 32482424.
Chandra Vemulapalli K, Pechero GR, Warner SJ, Achor TS, Gary JL, Munz JW, Choo AM, Prasarn ML, Chip Routt ML Jr. Is retrograde nailing superior to lateral locked plating for complete articular distal femur fractures? Injury. 2022;53(2):640–4. Epub 2021 Nov 23. PMID: 34863509.
Download references
Acknowledgements
We gratefully acknowledge the valuable contributions of Judas Kelley and Kelsey Hideshima in the oversight of this project, along with the insightful feedback provided by Megan Terle, Gillian Soles, Sean T. Campbell, Ellen Fitzpatrick, and Mark A. Lee during the review process of this manuscript.
No funding was used for this study. For the remaining authors there are no relevant conflicts of interest.
Author information
Authors and affiliations.
Department of Orthopaedic Surgery, University of California Davis, 4860 Y Street, Suite 3800, Sacramento, CA, 95817, USA
Shana Kong, Shannon Tse, Aziz Saade, Barry Bautista, Max Haffner & Augustine M. Saiz Jr.
You can also search for this author in PubMed Google Scholar
Contributions
A.M.S. devised the study and directed the project. S.K. and B.B. contributed to data collection, analysis, study interpretation, and manuscript drafting. M.H., S.T., A.S., A.M.S. were involved in project oversight, study interpretation, and manuscript drafting.
Corresponding author
Correspondence to Augustine M. Saiz Jr. .
Ethics declarations
Conflict of interest.
The authors declare the following financial interests/personal relationships which may be considered potential competing interests: AMS: OTA: committee member; AAOS: committee member; ORS: committee member; AO North America: committee member.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Kong, S., Tse, S., Saade, A. et al. Clinical differences between periprosthetic and native distal femur fractures: a comparative observational study. J Orthop Surg Res 19 , 303 (2024). https://doi.org/10.1186/s13018-024-04796-8
Download citation
Received : 07 March 2024
Accepted : 14 May 2024
Published : 20 May 2024
DOI : https://doi.org/10.1186/s13018-024-04796-8
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Journal of Orthopaedic Surgery and Research
ISSN: 1749-799X
- Submission enquiries: [email protected]
A deep transcriptome meta-analysis reveals sex differences in multiple sclerosis
Affiliations.
- 1 Bioinformatics and Biostatistics Unit, Principe Felipe Research Center (CIPF), 46012 Valencia, Spain.
- 2 Foundation Valencian Institute of Oncology (FIVO), 46009 Valencia, Spain.
- 3 Bioinformatics and Biostatistics Unit, Principe Felipe Research Center (CIPF), 46012 Valencia, Spain; Faculty of Health Sciences, San Jorge University, 50830 Zaragoza, Spain.
- 4 Instituto de Investigación Sanitaria Puerta de Hierro-Segovia de Arana (IDIPHISA), Grupo de Investigación en Linfomas, C/Joaquín Rodrigo 2, Majadahonda, 28222 Madrid, Spain.
- 5 Biomedical Imaging Unit FISABIO-CIPF, Fundación para el Fomento de la Investigación Sanitaria y Biomédica de la Comunidad Valenciana, 46012 Valencia, Spain.
- 6 Department of Pharmacology, Center for Genetic Medicine, Northwestern University Feinberg School of Medicine, Chicago, IL, USA.
- 7 Bioinformatics and Biostatistics Unit, Principe Felipe Research Center (CIPF), 46012 Valencia, Spain. Electronic address: [email protected].
- PMID: 37023829
- DOI: 10.1016/j.nbd.2023.106113
Background: Multiple sclerosis (MS), a chronic auto-immune, inflammatory, and degenerative disease of the central nervous system, affects both males and females; however, females suffer from a higher risk of developing MS (2-3:1 ratio relative to males). The precise sex-based factors influencing risk of MS are currently unknown. Here, we explore the role of sex in MS to identify molecular mechanisms underlying observed MS sex differences that may guide novel therapeutic approaches tailored for males or females.
Methods: We performed a rigorous and systematic review of genome-wide transcriptome studies of MS that included patient sex data in the Gene Expression Omnibus and ArrayExpress databases following PRISMA statement guidelines. For each selected study, we analyzed differential gene expression to explore the impact of the disease in females (IDF), in males (IDM) and our main goal: the sex differential impact of the disease (SDID). Then, for each scenario (IDF, IDM and SDID) we performed 2 meta-analyses in the main tissues involved in the disease (brain and blood). Finally, we performed a gene set analysis in brain tissue, in which a higher number of genes were dysregulated, to characterize sex differences in biological pathways.
Results: After screening 122 publications, the systematic review provided a selection of 9 studies (5 in blood and 4 in brain tissue) with a total of 474 samples (189 females with MS and 109 control females; 82 males with MS and 94 control males). Blood and brain tissue meta-analyses identified, respectively, 1 (KIR2DL3) and 13 (ARL17B, CECR7, CEP78, IFFO2, LOC401127, NUDT18, RNF10, SLC17A5, STMP1, TRAF3IP2-AS1, UBXN2B, ZNF117, ZNF488) MS-associated genes that differed between males and females (SDID comparison). Functional analyses in the brain revealed different altered immune patterns in females and males (IDF and IDM comparisons). The pro-inflammatory environment and innate immune responses related to myeloid lineage appear to be more affected in females, while adaptive responses associated with the lymphocyte lineage in males. Additionally, females with MS displayed alterations in mitochondrial respiratory chain complexes, purine, and glutamate metabolism, while MS males displayed alterations in stress response to metal ion, amine, and amino acid transport.
Conclusion: We found transcriptomic and functional differences between MS males and MS females (especially in the immune system), which may support the development of new sex-based research of this disease. Our study highlights the importance of understanding the role of biological sex in MS to guide a more personalized medicine.
Keywords: Biomarkers; Functional profiling; Meta-analysis; Multiple sclerosis; Neurodegeneration; Sex-based differences.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Publication types
- Meta-Analysis
- Research Support, Non-U.S. Gov't
- Carrier Proteins
- Cell Cycle Proteins
- Central Nervous System
- Gene Expression Profiling
- Multiple Sclerosis* / genetics
- Sex Characteristics
- Transcriptome*
- RNF10 protein, human
- CEP78 protein, human
Grants and funding
- R01 CA229618/CA/NCI NIH HHS/United States
IMAGES
VIDEO
COMMENTS
Types of Research Designs Compared | Guide & Examples. Published on June 20, 2019 by Shona McCombes.Revised on June 22, 2023. When you start planning a research project, developing research questions and creating a research design, you will have to make various decisions about the type of research you want to do.. There are many ways to categorize different types of research.
The guidance notes that the major difference between research and non-research lies in the primary intent of the activity. The primary intent of research is to generate or contribute to generalizable knowledge. The primary intent of non-research in public health is to prevent or control disease or injury and improve health, or to improve a ...
This type of research is subdivided into two types: Technological applied research: looks towards improving efficiency in a particular productive sector through the improvement of processes or machinery related to said productive processes. Scientific applied research: has predictive purposes. Through this type of research design, we can ...
The main difference between quantitative and qualitative research is the type of data they collect and analyze. ... Qualitative research, on the other hand, collects non-numerical data such as words, images, and sounds. The focus is on exploring subjective experiences, opinions, and attitudes, often through observation and interviews. ...
There are two main types of nonexperimental research designs: comparative design and correlational design. In comparative research, the researcher examines the differences between two or more groups on the phenomenon that is being studied. For example, studying gender difference in learning mathematics is a comparative research.
This clip from the Health Sciences Library's Introduction to Literature Searching workshop describes the difference between research and non-research articles. Primary and secondary research is briefly discussed. Tags. University of Cincinnati Libraries PO Box 210033, Cincinnati, Ohio 45221-0033
quandary over whether the activity is research or non-research. The key word in the regulations= definition of research for the purpose of classifying public health activities as either research or non-research is Adesigned.@ The major difference between research and non-research lies in the primary intent of the activity. The primary intent of
A research design is a strategy for answering your research question using empirical data. Creating a research design means making decisions about: Your overall research objectives and approach. Whether you'll rely on primary research or secondary research. Your sampling methods or criteria for selecting subjects. Your data collection methods.
Research conducted for the purpose of contributing towards science by the systematic collection, interpretation and evaluation of data and that, too, in a planned manner is called scientific research: a researcher is the one who conducts this research. The results obtained from a small group through scientific studies are socialised, and new ...
Nonscientific research is acquiring knowledge and truths about the world using techniques that do not follow the scientific method. For instance, Plato was a large proponent of some of these, and ...
Non-experimental research is research that lacks the manipulation of an independent variable. Rather than manipulating an independent variable, researchers conducting non-experimental research simply measure variables as they naturally occur (in the lab or real world). Most researchers in social sciences consider the distinction between ...
The major difference between research and non-research lies in the purpose of the activity. The purpose of research is to increase scientific knowledge. The purpose of non-research in public health is to prevent or control disease or injury and improve health, or to improve a public health program or service.
One distinction worth making between two types of non-experimental research is the difference be- tween quasi-experimental research and case studies. The example I discussed earlier - in which we wanted to examine incidence of lung cancer among smokers and non-smokers, without trying to control who smokes and who doesn't - is a quasi ...
An experiment is a study in which the researcher manipulates the level of some independent variable and then measures the outcome. Experiments are powerful techniques for evaluating cause-and-effect relationships. Many researchers consider experiments the "gold standard" against which all other research designs should be judged. Experiments are ...
While there are articles that can be published in academic journals that are 5 pages or less, these do not usually represent in-depth research. 5. Style. The writing style is theoretical rather than practical. The theoretical perspective means that a contribution to the existing body of research in the field is being made. 6. Audience
the research pertains to a non-causal relationship between variables. limited information can be accessed about the research subject. There are 3 main types of non-experimental research, namely; cross-sectional research, correlation research, and observational research. Cross-sectional Research
Examples. Discrete variables (aka integer variables) Counts of individual items or values. Number of students in a class. Number of different tree species in a forest. Continuous variables (aka ratio variables) Measurements of continuous or non-finite values. Distance.
This study investigated the differences in knowledge sharing (KS) behavior among academicians from research universities (RUs) and non-research universities (Non-RUs) and the impact of their differences on research engagement in Malaysia. From the lens of the theory of planned behavior, research engagement is integrated into the original theory as the consequence of KS behavior. Applying a ...
The aim of non-experimental research is to be descriptive, observational, and correlational and the aim is to either describe the situation or describe relationships. It looks at the correlation ...
The main difference between a research article and a non-research article is. a research article describes research by the original author. About us. About Quizlet; How Quizlet works; Careers; Advertise with us; Get the app; For students.
Finally, scientific research involves interpreting and trying to make sense of those data — going beyond the data themselves to draw conclusions about the underlying phenomenon being studied. Driving the whole research endeavor are one or more research problems or questions that the researcher is trying to address and potentially solve. In ...
There are two main types of research: non-experimental and experimental. It's critical to understand the advantages and disadvantages of each type in order to choose which is best for your research goals.. Experimental research is a type of quantitative research that controls the variables in order to test a hypothesis. Non-experimental research does not control the variables but instead ...
One distinction worth making between two types of non-experimental research is the difference between quasi-experimental research and case studies. The example I discussed earlier - in which we wanted to examine incidence of lung cancer among smokers and non-smokers, without trying to control who smokes and who doesn't - is a quasi ...
A key role of public health policy-makers and practitioners is to ensure beneficial interventions are implemented effectively enough to yield improvements in public health. The use of evidence to guide public health decision-making to achieve this is recommended. However, few studies have examined the relative value, as reported by policy-makers and practitioners, of different broad research ...
Voices in Bioethics is currently seeking submissions on philosophical and practical topics, both current and timeless. Papers addressing access to healthcare, the bioethical implications of recent Supreme Court rulings, environmental ethics, data privacy, cybersecurity, law and bioethics, economics and bioethics, reproductive ethics, research ethics, and pediatric bioethics are sought.
The main difference between research and non-research is<br>1). the type of skills we use to discover something.<br>2). the utilization of acceptable scientific methodology to solve problems to create new knowledge.<br>3). the quantitative and qualitative methods that are to be used.<br>4). all the above. The main difference between research ...
Research has shown critical individual differences in vulnerability to attributing incentive salience to drug cues, and that vulnerable individuals are at much higher risk for addiction. Moreover, combining incentive sensitization with poor cognitive control (e.g., during a drinking episode) makes for a "potentially disastrous combination ...
Introduction The incidence of periprosthetic distal femur fractures (PDFF) is increasing as the number of total knee replacements becomes more common. This study compared the demographics, fracture characteristics, treatment, and outcomes of periprosthetic versus native distal femur fractures (NDFF). Materials and methods This was a retrospective cohort study of patients ≥ 18 who underwent ...
Conclusion: We found transcriptomic and functional differences between MS males and MS females (especially in the immune system), which may support the development of new sex-based research of this disease. Our study highlights the importance of understanding the role of biological sex in MS to guide a more personalized medicine.